66 - Luteinizing Hormone Levels in Pubertal Children with CKD and Association with Change in GFR
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 66 Publication Number: 66.341
Hannah Kim, Pennsylvania State University College of Medicine, Hershey, PA, United States; Matthew Matheson, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States; Meredith Atkinson, Johns Hopkins University School of Medicine, Baltimore, MD, United States
Assistant Professor of Pediatrics Pennsylvania State University College of Medicine Hershey, Pennsylvania, United States
Background: Puberty is a period of marked change including development of secondary sexual characteristics, acceleration of linear growth, and development of reproductive capability.[1] Pubertal onset is initially marked by an increase in luteinizing hormone (LH) levels followed by physical changes. However, children with chronic kidney disease may have alterations in the hypothalamic-pituitary-gonadal axis due to the predominantly renal metabolism of several hormones involved in pubertal maturation. Further, pubertal onset as defined by physical changes has been associated with faster decline in glomerular filtration rate (GFR).[2]
Objective: We aimed to describe LH levels in children with CKD and its association with pubertal onset as well as change in GFR.
Design/Methods: We used prospective data from the Chronic Kidney Disease in Children (CKiD) study to describe timing of pubertal onset as defined by LH level greater than or equal to 0.3 IU/L. We used a mixed effects model with random intercept and random slope to compare the slope of decline of GFR before and after pubertal onset as determined by LH level. The model was adjusted for age, glomerular disease diagnosis, baseline proteinuria on the log scale, and BMI category.
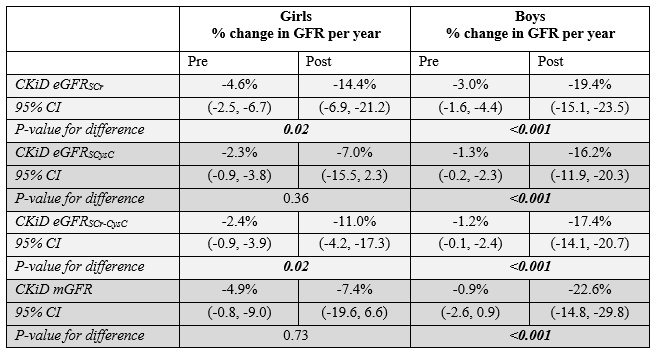
Results: There were 89 children who were followed through pubertal onset as determined by LH. There was reasonable agreement between LH level and clinical demonstration of pubertal onset as determined by Tanner stage when assessed using percent agreement (85% and 82% respectively for girls and boys), percent positive agreement (77% and 76% respectively for girls and boys), and kappa (0.684 and 0.602 for girls and boys respectively). The mixed effects model showed faster decline in GFR in both girls and boys pre- versus post-pubertal onset using LH as a marker of pubertal onset (p < 0.001 for boys). Conclusion(s): Although LH is predominantly renally metabolized, there is reasonable agreement between LH level and clinical pubertal onset as determined by Tanner stage in children with CKD. There is a faster decline in GFR seen in both girls and boys using LH as a marker of pubertal onset which occurs prior to the pubertal growth spurt. Clinicians should be aware that puberty is a high-risk period for GFR decline. Table 1. Clinical characteristics at pubertal onset as defined by luteinizing hormone level Table 2. Average GFR percent change before and after pubertal onset for girls and boys with pubertal onset as defined by luteinizing hormone level from a mixed effects model adjusted for age, BMI, glomerular disease diagnosis, and baseline proteinuria on a log scale


.png)