73 - Relationship of Urine Uromodulin with Blood Pressure in Children with Chronic Kidney Disease
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 73 Publication Number: 73.341
Christine Bakhoum, Yale University, New Haven, CT, United States; Matthew Matheson, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States; Susan Furth, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Joachim H. Ix, University of California, San Diego School of Medicine, San Diego, CA, United States; Pranav Garimella, University of California, San Diego School of Medicine, La Jolla, CA, United States
Assistant Professor Yale University New Haven, Connecticut, United States
Background: Uromodulin, the most abundant protein in healthy urine, regulates activity of the sodium-potassium-two-chloride transporter (NKCC2) in the thick ascending limb of the loop of Henle. In adults without chronic kidney disease (CKD), high urine uromodulin levels have been associated with greater rise in blood pressure in response to salt.
Objective: We hypothesized that higher urine uromodulin levels would be associated with higher blood pressure in children with CKD and that there would be an interaction of dietary sodium on this association.
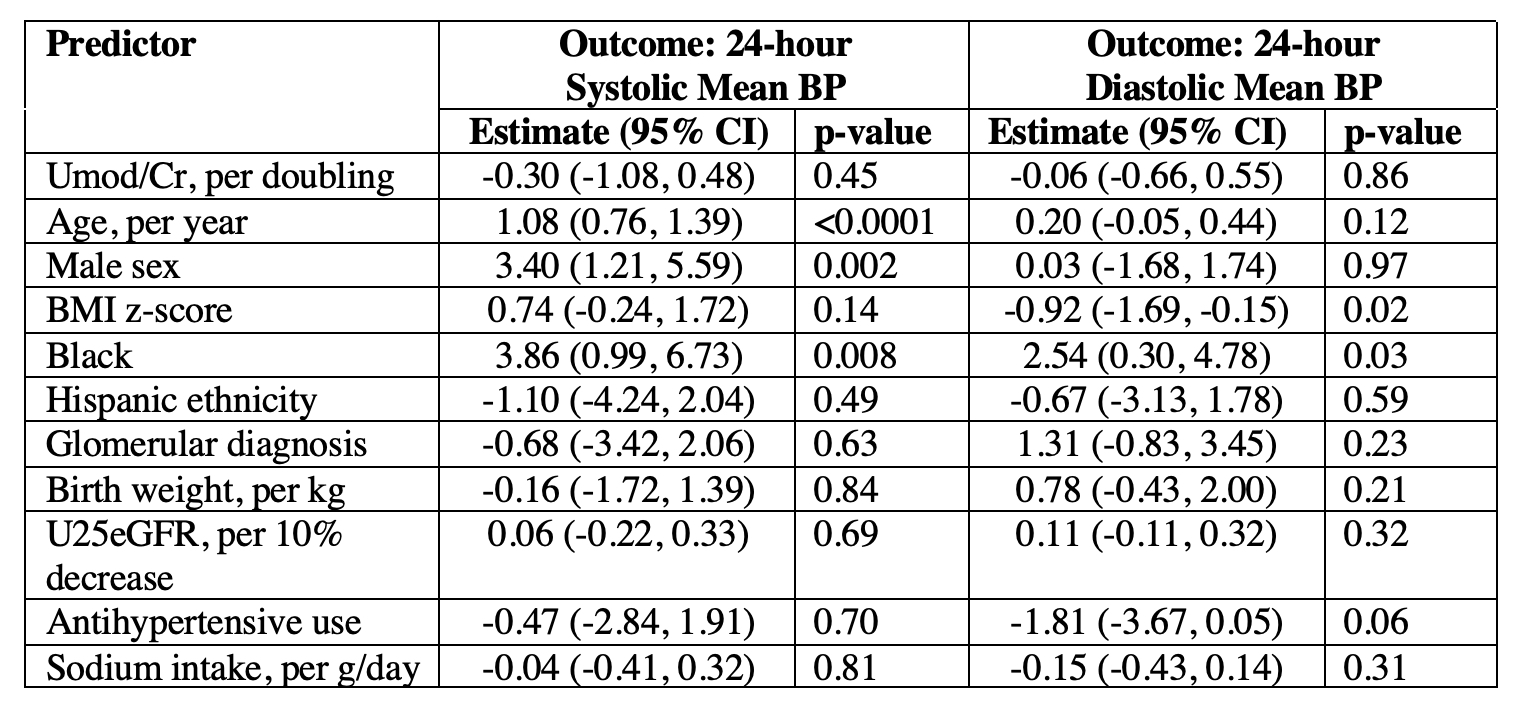
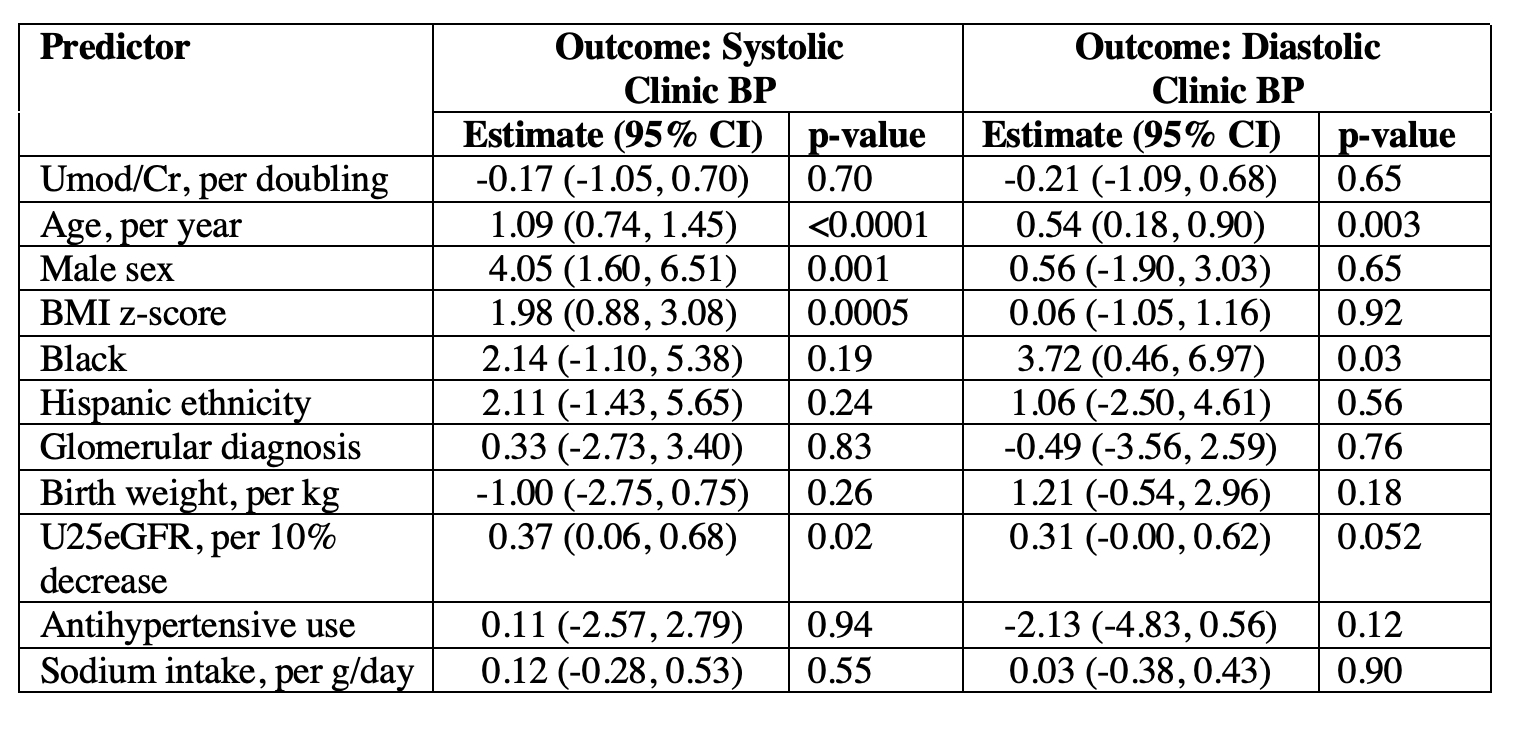
Design/Methods: In the CKD in Children (CKiD) Cohort, we utilized multivariable linear regression models to evaluate the relationship between baseline spot urine uromodulin levels indexed to creatinine (Umod/Cr mg/g) and 24-hour mean systolic and diastolic blood pressure. Using the same method, we evaluated the relationship between Umod/Cr (mg/g) and baseline clinic blood pressure. We log2 – transformed Umod/Cr (mg/g) given its skewed distribution and tested whether sodium intake (g/day), based on food frequency questionnaire, modified the association of uromodulin and blood pressure.
Results: Among a total of 436 participants, the median age was 12.4 years [8.9, 15.2], median eGFR was 50 ml/min/1.73 m2 [36, 62] and median 24-hour mean systolic blood pressure was 112 mmHg [104, 119]. The etiology of CKD was glomerular disease in 27%. The median Umod/Cr level was 0.118 mg/g [IQR 0.048, 0.225]. Each doubling of Umod/Cr ratio was associated with 0.30 mmHg (-1.08, 0.48) and 0.06 mmHg (-0.66, 0.55) lower 24-hour systolic and diastolic mean blood pressure, respectively (Table 1). Each doubling of Umod/Cr ratio was associated with 0.17 mmHg (-1.05, 0.70) and 0.21 mmHg (-1.09, 0.68) lower clinic systolic and diastolic blood pressure, respectively (Table 2). These relationships were not statistically significant, and we did not find a significant interaction between uromodulin levels and sodium intake (p > 0.05 in all models).Conclusion(s): Urine uromodulin levels are not associated with blood pressure in the CKiD cohort. We did not identify a significant interaction between uromodulin levels and sodium intake. Table 1. Multivariable linear regression model evaluating the relationship of baseline urine uromodulin levels with 24-hour mean systolic and diastolic blood pressure. Table 2. Multivariable linear regression model evaluating the relationship of baseline urine uromodulin levels with clinic systolic and diastolic blood pressure.