
Nephrology: CKD
Category: Abstract Submission
Nephrology III: General Nephrology and Dialysis
William E. Smoyer, MD
Vice President, Clinical and Translational Research
Nationwide Children's Hospital
Bexley, Ohio, United States
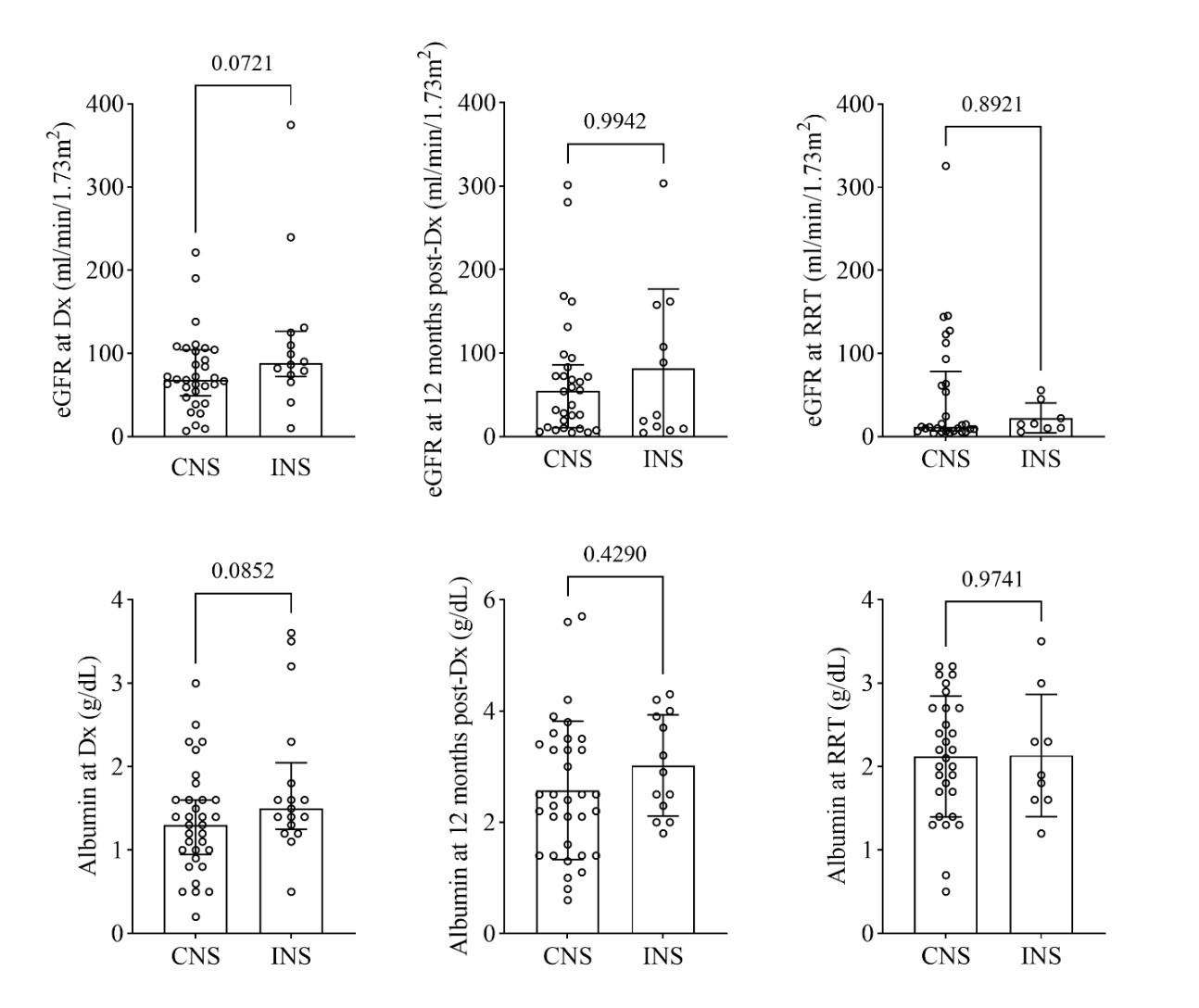 Dx = diagnosis; RRT = renal replacement therapy
Dx = diagnosis; RRT = renal replacement therapy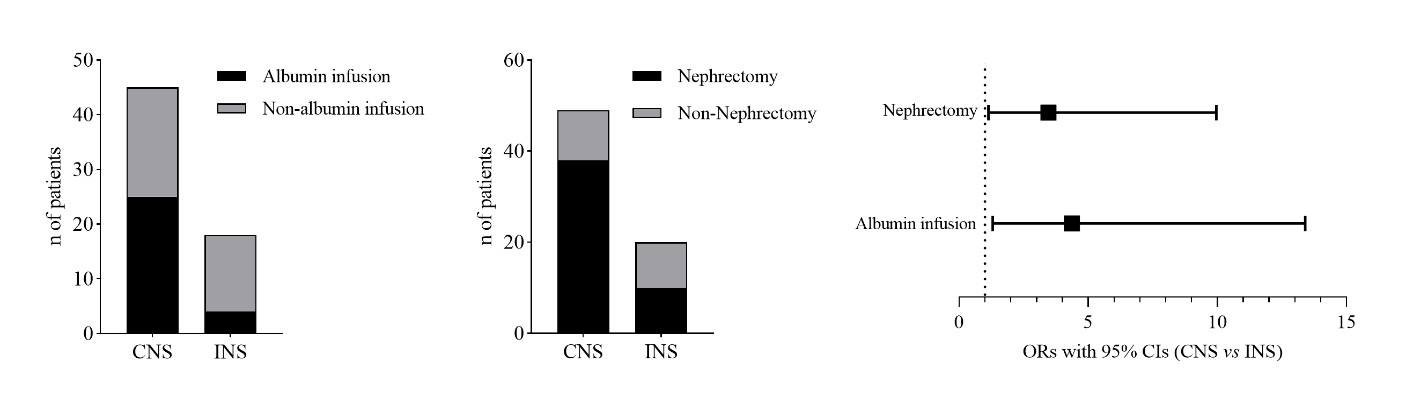 Nx = nephrectomy; RRT = renal replacement therapy
Nx = nephrectomy; RRT = renal replacement therapy