618 - Who, Where, When: Decisions for Extremely Early Deliveries
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 618 Publication Number: 618.306
Danielle LoRe, NewYork-Presbyterian Morgan Stanley Children's Hospital, New York, NY, United States; Catherine M. Groden, Indiana University School of Medicine, Indianapolis, IN, United States; Allison Schuh, Comer Children's Hospital at University of Chicago Medical Center, Chicago, IL, United States; Maggie M. Vogel, Advocate Children's Hospital - Oak Lawn, Oak Lawn, IL, United States; Aunum Akhter, University of Michigan Medical School, Ann Arbor, MI, United States; Sanela Andelija, HCA Healthcare/USF Morsani College of Medicine GME Programs, Brandon Regional Hospital, Brandon, FL, United States; Jasmine Soo, Indiana University School of Medicine, Indianapolis, IN, United States; Shelley Hoffman, Indiana University School of Medicine, Indianapolis, IN, United States; Christine Carlos, University of Chicago Division of the Biological Sciences The Pritzker School of Medicine, Chicago, IL, United States; Tiffany Tonismae, Johns Hopkins All Children's Hospital, Tampa, FL, United States; Naomi T. Laventhal, University of Michigan Medical School, Ann Arbor, MI, United States; Richard Kampanatkosol, Advocate Children's Hospital - Oak Lawn, Oak Lawn, IL, United States; Bree Andrews, University of Chicago Division of the Biological Sciences The Pritzker School of Medicine, Chicago, IL, United States; Brownsyne Tucker Edmonds, Indiana University School of Medicine, Department Of Ob/Gyn, Indianapolis, IN, United States; Kathleen G. Brennan, Columbia University Vagelos College of Physicians and Surgeons, New York, NY, United States; Dalia M. Feltman, NorthShore University HealthSystem Evanston Hospital, Burr Ridge, IL, United States
Neonatal-Perinatal Fellow Indiana University School of Medicine Indiana University School of Medicine Indianapolis, Indiana, United States
Background: Drivers of differences in resuscitation and survival rates of the most premature infants are not understood, but these differences may reflect inequities in care. The INDEED (Investigating Neonatal Decisions for Extremely Early Deliveries) group is analyzing resuscitation factors for mothers delivering between 22 and 24 weeks’ gestation at 15 U.S. centers in the last 10 years.
Objective: To understand differences in medical and sociodemographic factors, delivery center, and year between mothers whose extremely early newborns did or did not receive delivery room resuscitation.
Design/Methods: We reviewed data from 7 centers from 2011-2020. Mothers presenting with living fetuses without severe anomalies who delivered at 22 0/7 to 24 6/7 weeks’ gestation were included. Sociodemographic, obstetric management, consultation, and neonatal outcome data were collected. Federal census-related geocoding data (2015 American Community Survey 5-year estimates) were extracted using mothers’ residential zip codes. Characteristics were compared: 1) mothers grouped by whether their liveborn infants received delivery room attempted resuscitation (AR) or comfort care (CC); 2) centers grouped by higher (HR) and lower (LR) attempted resuscitation rates. Significantly different (p < 0.05) characteristics were included in multivariable logistic regression analyses for each comparison group. Rates of mothers with live births and resuscitated newborns were also compared between two epochs: 2011-2015 vs. 2016-2020.
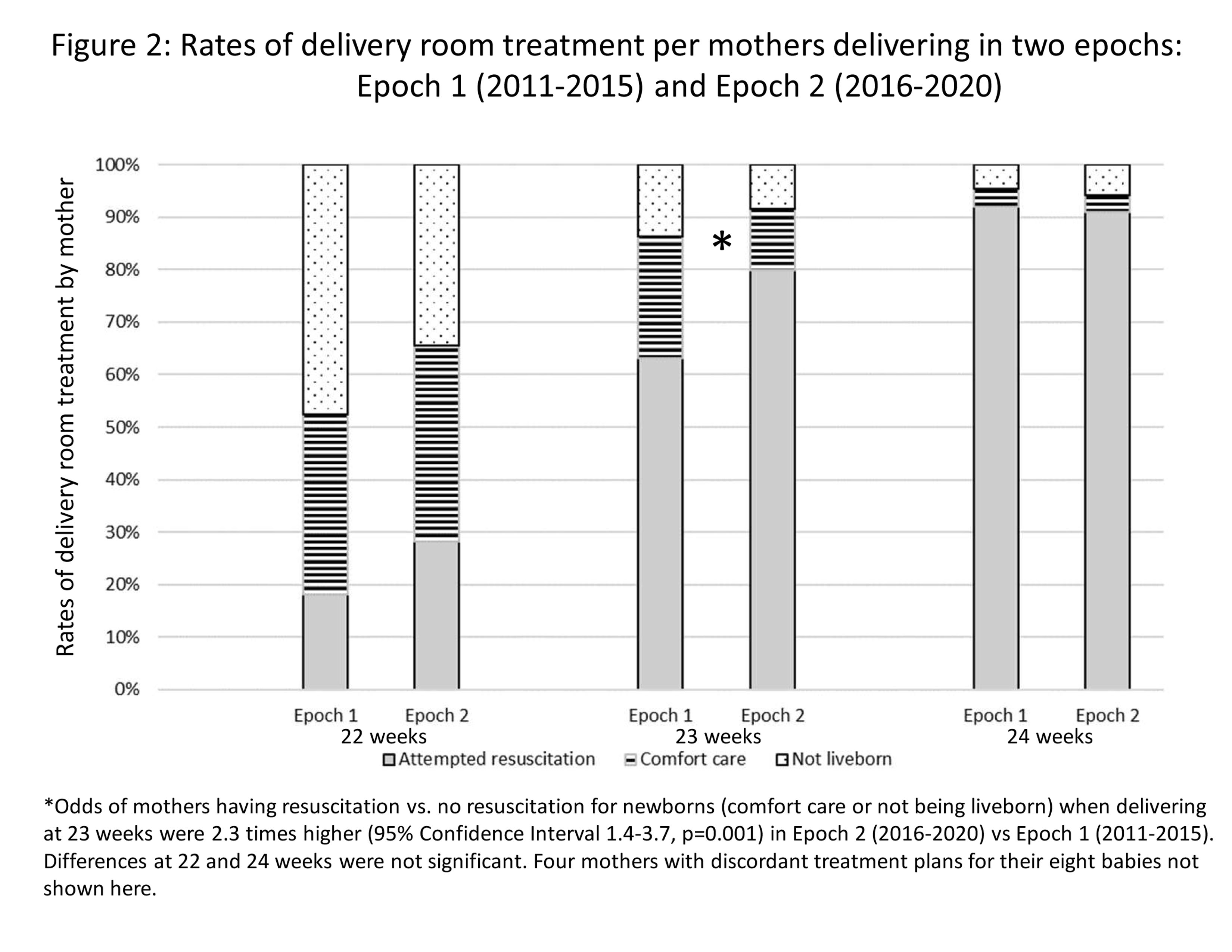
Results: 905 mothers and 1030 babies were included (Figure 1). Attempted resuscitation for mothers delivering live newborns ranged between centers and by weeks’ gestation: 22 weeks 0-59%; 23 weeks 63-94%; 24 weeks 85-100%. Table 1 shows analyses of AR vs CC mothers and HR vs LR centers. AR vs. CC mothers were less likely to be primary English-speakers and more likely to be insured. HR vs. LR center mothers were more likely to be African American, prenatally transferred, and living in areas with higher rates of geocoded socioeconomic hardship markers, but less likely to be insured or have identified religions. Mothers delivering at 23 weeks in the more recent epoch had significantly higher rates of live birth and resuscitation (Figure 2).Conclusion(s): Resuscitation rates and delivery outcomes changed with time and by delivery center more than by maternal factors, suggesting care for extremely early newborns is not equitable. Our full dataset comprised of 15 centers will reveal targets for improving provision of equitable care as resuscitation practices change over time. LoRe CVLoRe_CV.pdf Figure 2. Rates of delivery room treatment per mothers delivering in two epochs: Epoch 1 (2011-2015) and Epoch 2 (2016-2020)