
General Pediatrics: All Areas
Category: Abstract Submission
General Pediatrics V

Amanda C. Esteves, MD
General Pediatric Patient Safety Fellow
Columbia University Irving Medical Center
Fort Lee, New Jersey, United States
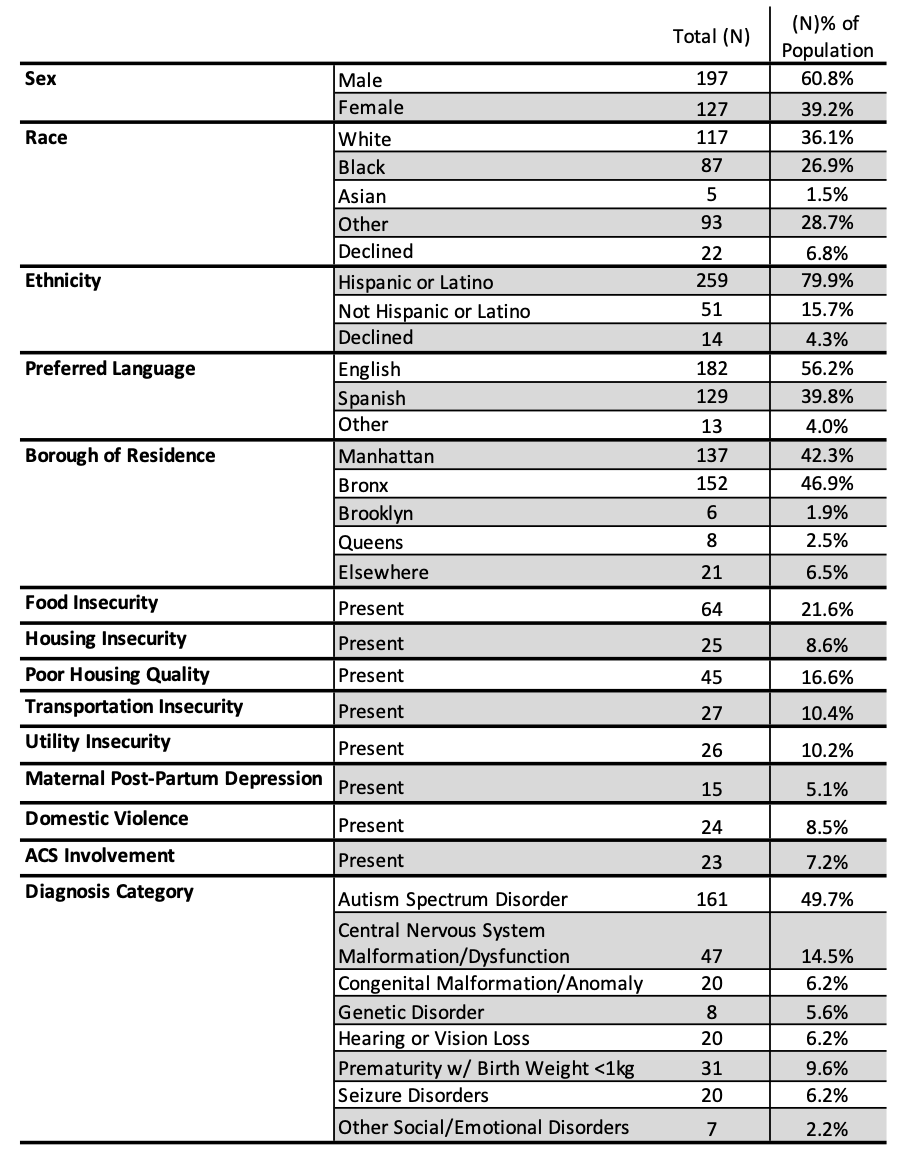 Study Population Demographic Characteristics
Study Population Demographic Characteristics.png) Rates of Referral, Evaluation, Service Receipt and Mean Time from First Referral to Service Receipt by Eligible Diagnosis
Rates of Referral, Evaluation, Service Receipt and Mean Time from First Referral to Service Receipt by Eligible Diagnosis