143 - Expanding Pediatric Surge Capacity and Capabilities: A Statewide Assessment
Monday, April 25, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 143 Publication Number: 143.416
Joyce Li, Boston Children's Hospital, Boston, MA, United States; Arianne Baker, Boston Children's Hospital, Boston, MA, United States; Gabrielle D'Ambrosi, Boston Children's Hospital, Allston, MA, United States; Michael C. Monuteaux, Boston Children's Hospital, Boston, MA, United States; Sarita Chung, Boston Children's Hospital, Boston, MA, United States
Assistant Professor Boston Children's Hospital Boston, Massachusetts, United States
Background: During surge events, hospitals need to know their capacity and capabilities beyond their typical facility and operating procedures. As mass casualty and other disaster events are uncommon, hospitals’ pediatric surge capacities and capabilities are frequently unknown.
Objective: To describe inpatient capacity and critical care and subspecialty capabilities for children during normal and surge operating conditions.
Design/Methods: We performed a mixed methods study utilizing data from two sources. To calculate hospital-level pediatric licensed inpatient and intensive care unit (ICU) care capacity, we utilized the Massachusetts Department of Public Health licensing records for inpatient beds. To assess pediatric policies, staffing, and service availability during both normal operations and surge scenarios, we performed a state-wide survey of all Massachusetts acute care hospitals with inpatient services (pediatric and/or adult) and emergency departments. We calculated the frequencies of overall inpatient non-ICU and ICU care resources and capacity, staffing and subspecialty service availability, and pediatric surge policies during normal operations and surge situations.
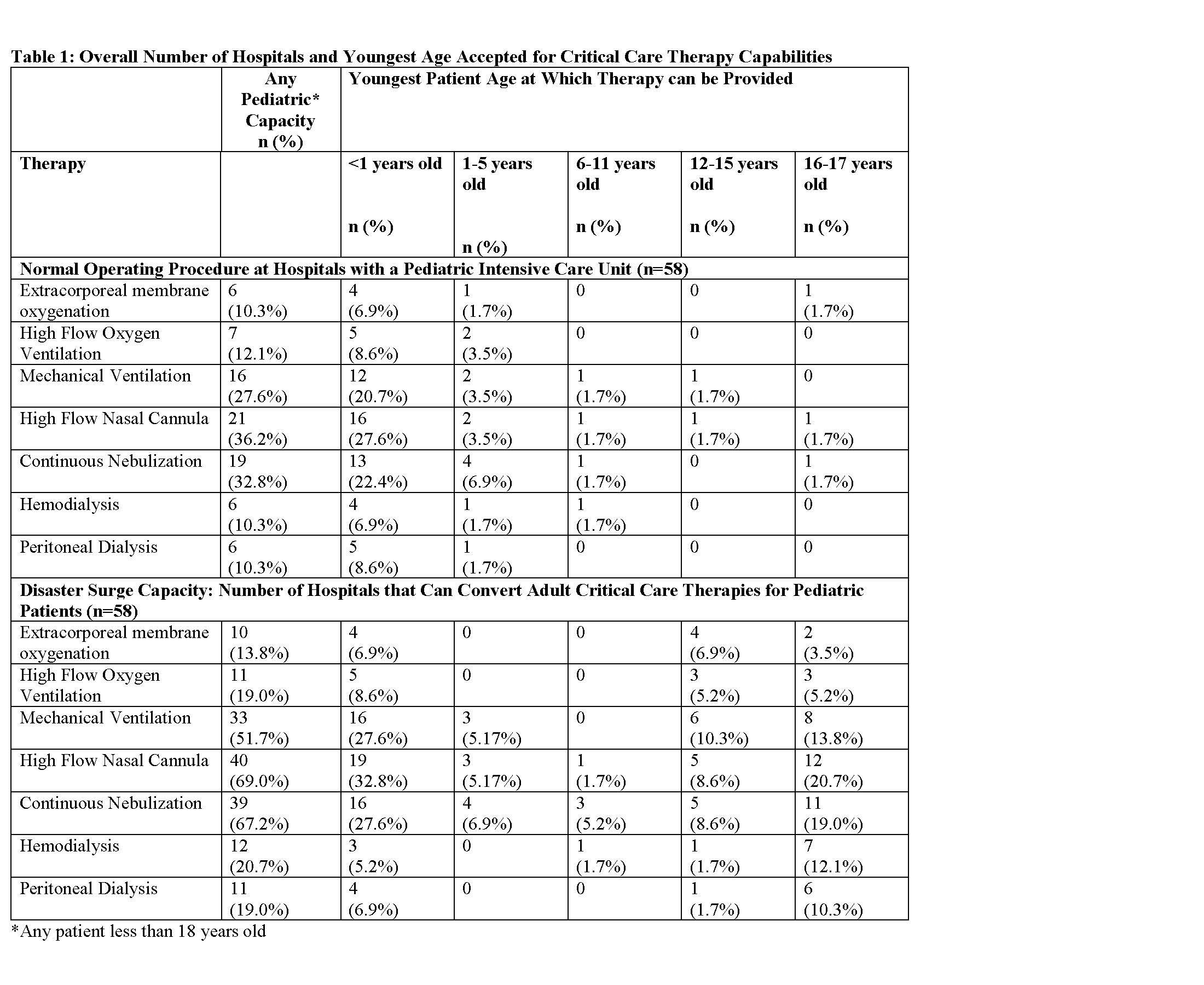
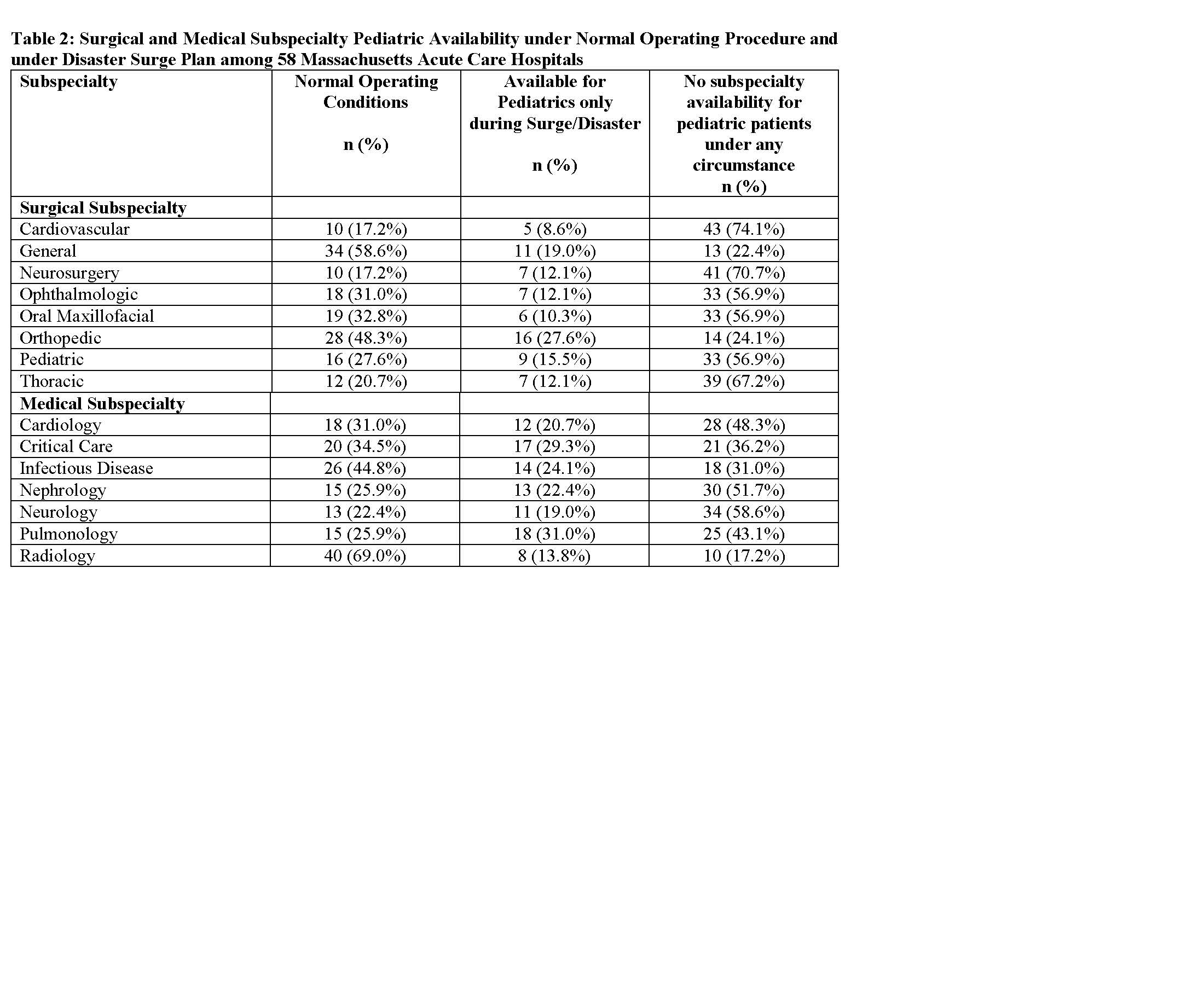
Results: We received survey responses from 58 out of 64 (91% of Massachusetts acute care hospitals) with the majority of surveys completed by emergency management leadership (n=45; 78%). Of the 58 included acute care hospitals, 21% had low emergency department pediatric volume ( < 1800 patients/year as defined by Emergency Medical Services for Children), 29% medium-low (1801-4999 patients/year) and 29% medium-high (5000-9999 patients/year), and 21% high (≥ 10,000 patients/year). On a statewide level, 67 non-ICU adult beds and 33 adult ICU beds could convert to pediatric critical care beds during a pediatric surge. Under normal operating procedures, only 21 (36% of acute care hospitals) had pediatric critical care capabilities, but the majority (n=41; 69%) could convert adult to pediatric critical care capacities during a surge (Table 1). Statewide, pediatric subspecialist availability was limited during normal operations but could expand during a disaster (Table 2). Only 13 (22%) hospitals have a surge plan that includes pediatric patients.Conclusion(s): Massachusetts acute care hospitals have limited pediatric acute care capacity, although some facilities could re-purpose adult resources for the care of children during a pediatric surge allowing children to be cared for in their communities. Further research is needed to understand optimal statewide pediatric surge capacity. Table 1: Overall Number of Hospitals and Youngest Age Accepted for Critical Care Therapy Capabilities Table 2: Surgical and Medical Subspecialty Pediatric Availability under Normal Operating Procedure and under Disaster Surge Plan among 58 Massachusetts Acute Care Hospitals