71 - Potassium Status in Pediatric Chronic Kidney Disease: A Preliminary Report from the Chronic Kidney Diseases in Childhood (CKiD) Study
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 71 Publication Number: 71.341
Katherine Kurzinski, Children's Mercy Hospital, Kansas City, MO, United States; Yunwen Xu, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States; Derek K. Ng, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States; Susan Furth, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; George J. Schwartz, University of Rochester School of Medicine and Dentistry, Rochester, NY, United States; BRADLEY A. WARADY, CHILDREN'S MERCY KANSAS CITY, KANSAS CITY, MO, United States
Pediatric Nephrology Fellow Children's Mercy Hospital Kansas City, Missouri, United States
Background: Potassium trends are well described in adult chronic kidney disease (CKD) and hyperkalemia is known to be associated with increased disease progression, morbidity, and mortality. Large scale studies assessing potassium trends and the prevalence of hyperkalemia in pediatric CKD, however, have not been performed.
Objective: We aimed to characterize median serum potassium levels and the prevalence of hyperkalemia for each CKD stage using the CKiD cohort. The relationship of serum potassium and hyperkalemia with patient demographics, CKD etiology (glomerular or non-glomerular), presence of acidosis, and degree of proteinuria was also evaluated.
Design/Methods: Median serum potassium levels and the percentage of laboratory assessments in which hyperkalemia (K >5.5mmol/L) was detected were compared across CKD stages as estimated by the 2009 Bedside Schwartz or the 2012 Cystatin C-Creatinine CKiD equations. The Kruskal-Wallis test was used to compare median potassium levels across groups including sex, ethnicity, CKD etiology, presence of acidosis, and degree of proteinuria. Chi square tests were used to compare the percentage of assessments with hyperkalemia across the above groups.
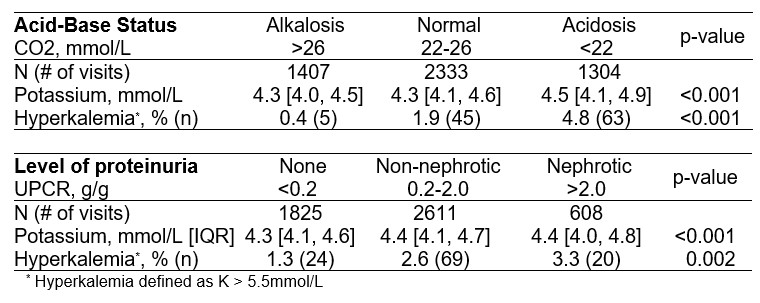
Results: Laboratory data from 5044 study visits conducted with 1038 patients were included. ACE inhibitor/ARB and diuretic usage was more common in patients with glomerular (79.2% and 46.6%) versus nonglomerular (11.5% and 4.0%) CKD (p < 0.001 for both). Median serum potassium levels and the percentage of patient assessments with hyperkalemia significantly increased with advancing CKD stage for patients with glomerular and nonglomerular CKD (Table 1). Acidosis (CO2 < 22mmol/L) and nephrotic-range proteinuria (UPCR >2.0) also resulted in higher median serum potassium levels and a significantly greater frequency of hyperkalemia when compared to assessments without acidosis or nephrotic-range proteinuria (Table 2). Whereas there was no difference in the percentage of study visits in which hyperkalemia was detected between females and males (2.1% versus 2.3%, p=0.730), hyperkalemia was significantly more common in Hispanic patients (3.6% versus 2.0% non-Hispanic, p=0.011). Conclusion(s): Within the CKiD cohort, patients with more advanced stages of CKD, acidosis, and nephrotic-range proteinuria had significantly higher median serum potassium levels and a higher percentage of laboratory assessments with hyperkalemia, irrespective of CKD etiology. This information can help identify those patients at greatest risk for substantial elevations of serum potassium who may benefit from dietary and/or medication interventions. Table 1. Median serum potassium levels and percentage of assessments with hyperkalemia by eGFR-based CKD stage Table 2. Median serum potassium levels and percentage of assessments with hyperkalemia by acid-base status and level of proteinuria

.jpg "Katherine Kurzinski, MD photo")
.jpg)