
Asthma
Category: Abstract Submission
Asthma

Geneva D. Mehta, MD
Clinical Fellow in Allergy and Immunology
Brigham and Women's Hospital
Boston, Massachusetts, United States
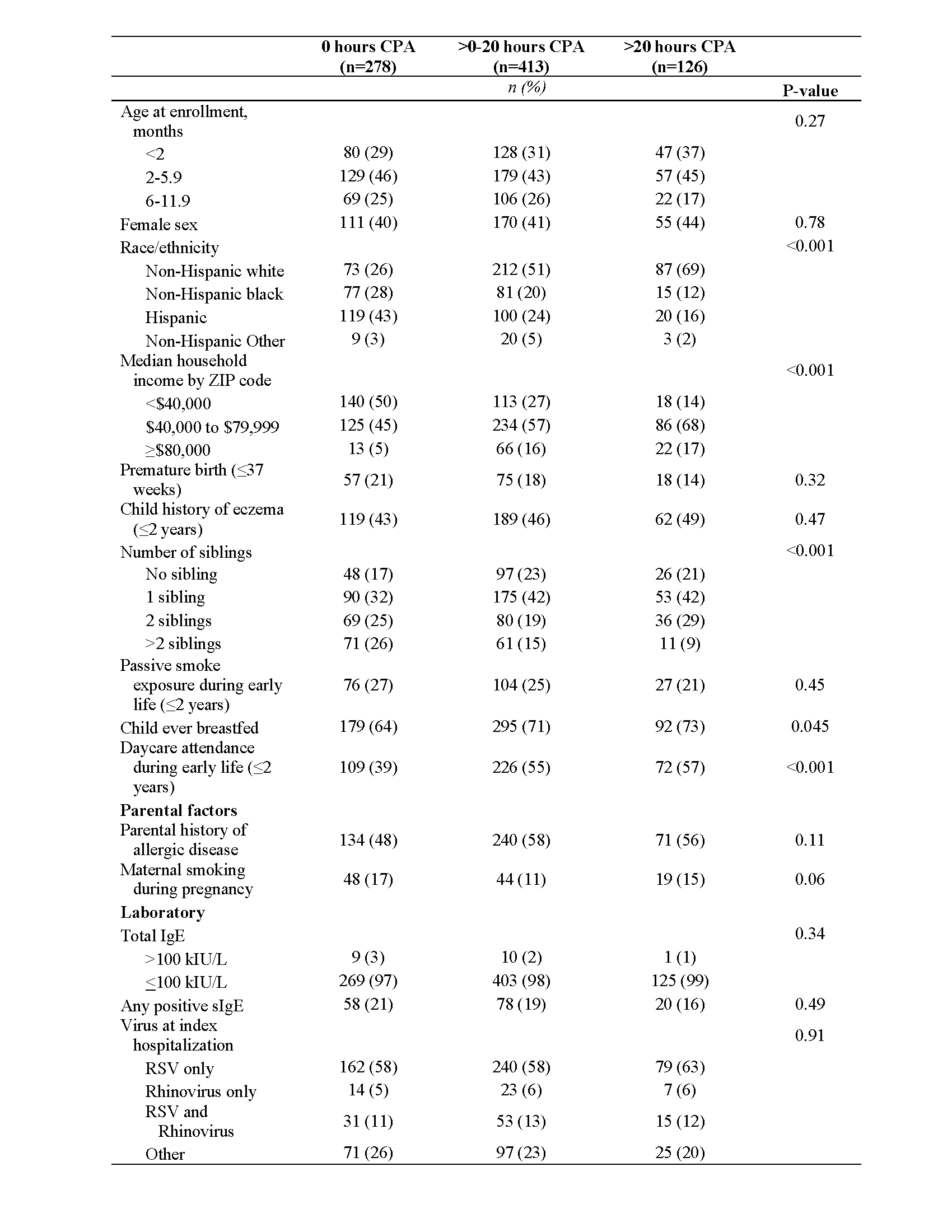 Abbreviations: CPA, cumulative pool attendance; IgE, immunoglobulin E; sIgE, serum specific-IgE; RSV, Respiratory Syncytial Virus.
Abbreviations: CPA, cumulative pool attendance; IgE, immunoglobulin E; sIgE, serum specific-IgE; RSV, Respiratory Syncytial Virus.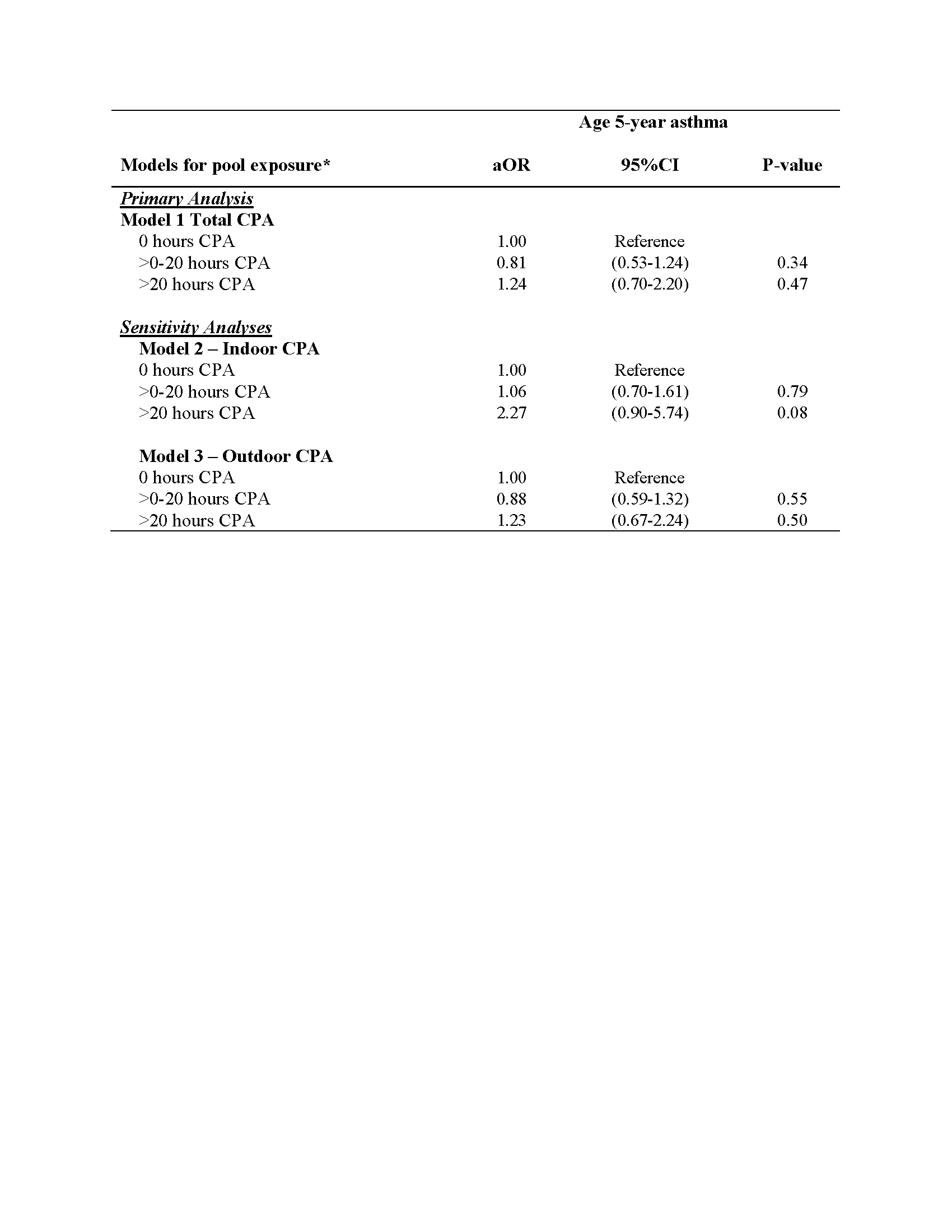 Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; CPA, cumulative pool
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; CPA, cumulative pool