510 - Necrotizing Enterocolitis (NEC) in Small for Gestational Age (GA) (SGA) Infants vs Appropriate for GA (AGA) Infants
Monday, April 25, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 510 Publication Number: 510.426
Mariela O. Sanchez Rosado, University of Texas Southwestern Medical School, Dallas, TX, United States; Jordan D. Reis, Baylor Scott & White, Prosper, TX, United States; Diksha Verma, University of Texas Southwestern Medical School, Dallas, TX, United States; isabelle M. Kiefaber, University of Texas Southwestern Medical School, Dallas, TX, United States; Patti J. Burchfield, University of Texas Southwestern Medical School, Dallas, TX, United States; Larry S. Brown, Parkland Health & Hospital System, Dallas, TX, United States; Luc P. Brion, University of Texas Southwestern Medical School, Dallas, TX, United States
Neonatal-Perinatal Medicine Fellow University of Texas Southwestern Medical School Dallas, Texas, United States
Background: NEC is a multifactorial disease that primarily affects preterm infants. Risk of NEC is associated with GA, birth weight (BW) and other factors. Additionally, timing of disease also seems to be related with GA and weight, with older GA and larger infants developing NEC earlier. SGA infants are at increased risk of developing NEC when compared to AGA infants.
Objective: To describe differences in timing of NEC development in SGA vs AGA infants. We also aim to describe risk or protective factors associated with NEC in our population.
Design/Methods: Retrospective cohort study of infants born at Parkland Hospital < 33 weeks GA or <1500g from 2009 up to June 2021. Demographic information such as GA, BW, growth status (AGA vs SGA), and delivery type were recorded. For infants identified as having NEC stage II or greater, additional information was obtained from their charts including date of NEC diagnosis, duration of mother’s own milk (MOM) and/or donor breastmilk (DBM) feedings, caloric density of feeds at time of NEC and episodes of sepsis or vasopressor use on the week of NEC diagnosis. Patients were divided into two main categories: SGA and AGA. Within each group, infants were also classified in subgroups by gestational age (23-28 weeks GA and 29-32 weeks GA). Mean post menstrual age (PMA) and median postnatal age (PNA) at time of NEC diagnosis were calculated for each subgroup. Days of MoM feeding were recorded from the electronic medical record. Prolonged duration of MoM was defined as still receiving MoM past the mean PMA of developing NEC within that GA category. Statistical analysis included ANOVA, Fisher’s exact test, and stepwise logistic regression.
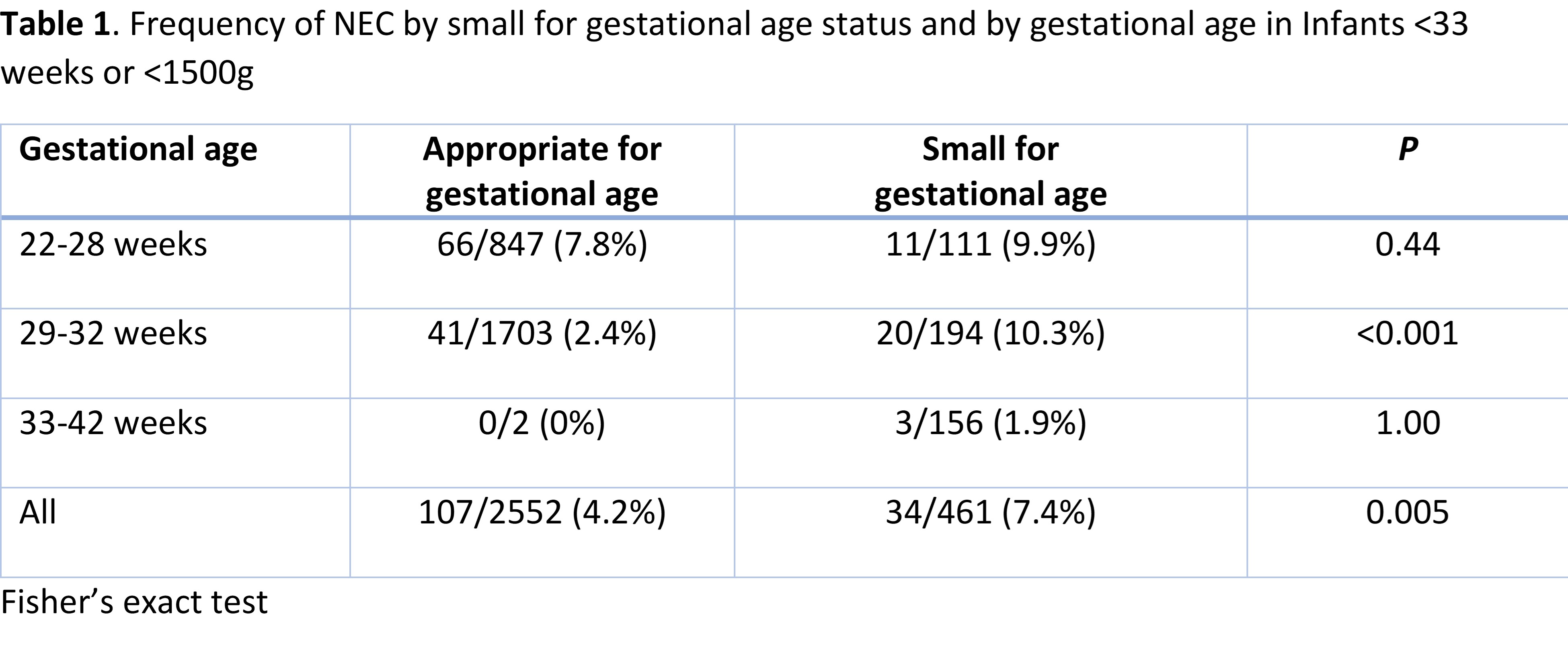
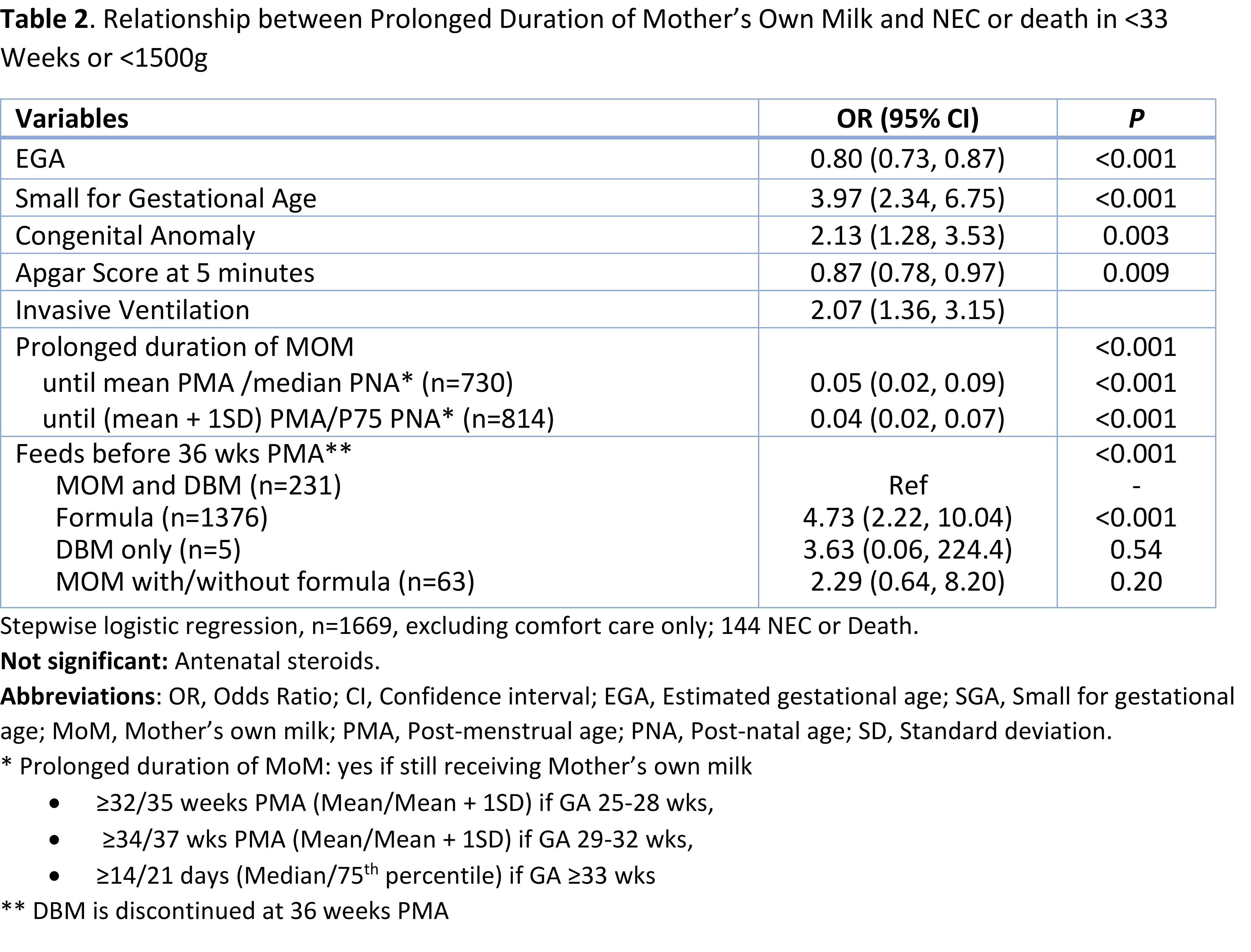
Results: Among 3012 infants, 142 developed NEC, with higher frequency in SGA than AGA among 29-32 weeks GA infants (Table 1). Factors associated with a decreased odds of NEC (not shown) and of NEC or death included GA, higher Apgar scores at 5 minutes and prolonged duration of MoM feedings (Table 2). Among infants < 33 weeks GA who developed NEC, 30 were SGA and 108 were AGA. SGA infants develop NEC at a later PMA and PNA when compared to AGA infants. Energy content of feeds before NEC were significantly higher in SGA than AGA (Table 3). However, energy content was similar in AGA and SGA infants when analyzed within groups of similar PNA when NEC developed ( < 10 days vs >10 days). Conclusion(s): NEC develops at a later PMA and PNA in SGA infants when compared to AGA infants. Prolonged duration of MoM feeding was associated with decreased odds of NEC and of NEC or death among our cohort. Table 1. Frequency of NEC by small for gestational age status and by gestational age in Infants < 33 weeks or < 1500g Table 2. Relationship between Prolonged Duration of Mother’s Own Milk and NEC or death in < 33 Weeks or < 1500g