Neonatal Infectious Diseases/Immunology
Category: Abstract Submission
Neonatal Infectious Diseases/Immunology: Sepsis
.jpg "Faris N. Al Gharaibeh, MD photo")
Faris N. Al Gharaibeh, MD
Clinical Fellow
Cincinnati Children's Hospital Medical Center
cincinnati, Ohio, United States
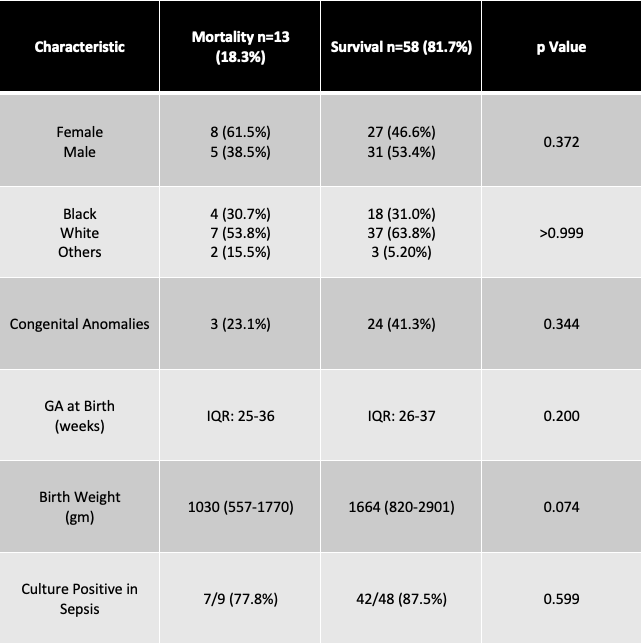 Neonates who experienced mortality at discharge were comparable to those who did not. There was a statistically insignificant trend for lower gestational age at birth and lesser weight in those who died compared to those who survived.
Neonates who experienced mortality at discharge were comparable to those who did not. There was a statistically insignificant trend for lower gestational age at birth and lesser weight in those who died compared to those who survived.