401 - Evaluating the Quality of Pediatric Care in Critical Access Hospital Emergency Departments
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 401 Publication Number: 401.315
Mary D. Patterson, University of Florida College of Medicine, Gainesville, FL, United States; Martha (Molly) W. Stevens, Larner School of Medicine, UVM, Division of Emergency Medicine, Burlington, VT, United States; Jessica Katznelson, Johns Hopkins School of Medicine, Baltimore, MD, United States
Johns Hopkins School of Medicine Johns Hopkins Baltimore, Maryland, United States
Background: Concerns have been raised about the quality of emergency care provided at rural hospitals. Metrics exist to measure the quality of care for adults, but there are no agreed upon metrics for pediatric patients. An implicit review tool has been developed and validated to serve as a way to qualitatively evaluate pediatric emergency care.
Critical Access Hospitals (CAH) are small rural institutions providing the only source of local emergency care. CAH Emergency Departments (ED) are staffed by providers with limited pediatric training. Little is known about the quality of care provided to pediatric patients in the CAH ED setting.
Objective: To use a validated tool from the pediatric literature to assess the quality of care provided to high acuity pediatric patients presenting to CAH ED.
Design/Methods: As part of a larger project, we reviewed the charts of 101 consecutive patients < 18 yr who presented to 3 CAH ED with a primary medical complaint and who were triaged at the highest acuity levels (Emergency Severity Index 1 or 2) over 12 months. The implicit review tool consists of 5 stages of care domains and an overall composite score, with each domain graded on a scale of 1 (worst) to 7 (best). The tool was completed independently by two pediatric emergency medicine (PEM) board certified providers who did an in depth chart review for each patient. The average score for the two reviewers was calculated for each category and overall. If the final score differed by more than 2 between the providers, a 3rd PEM boarded physician reviewed the charts and scores were calculated as the average of the 3.
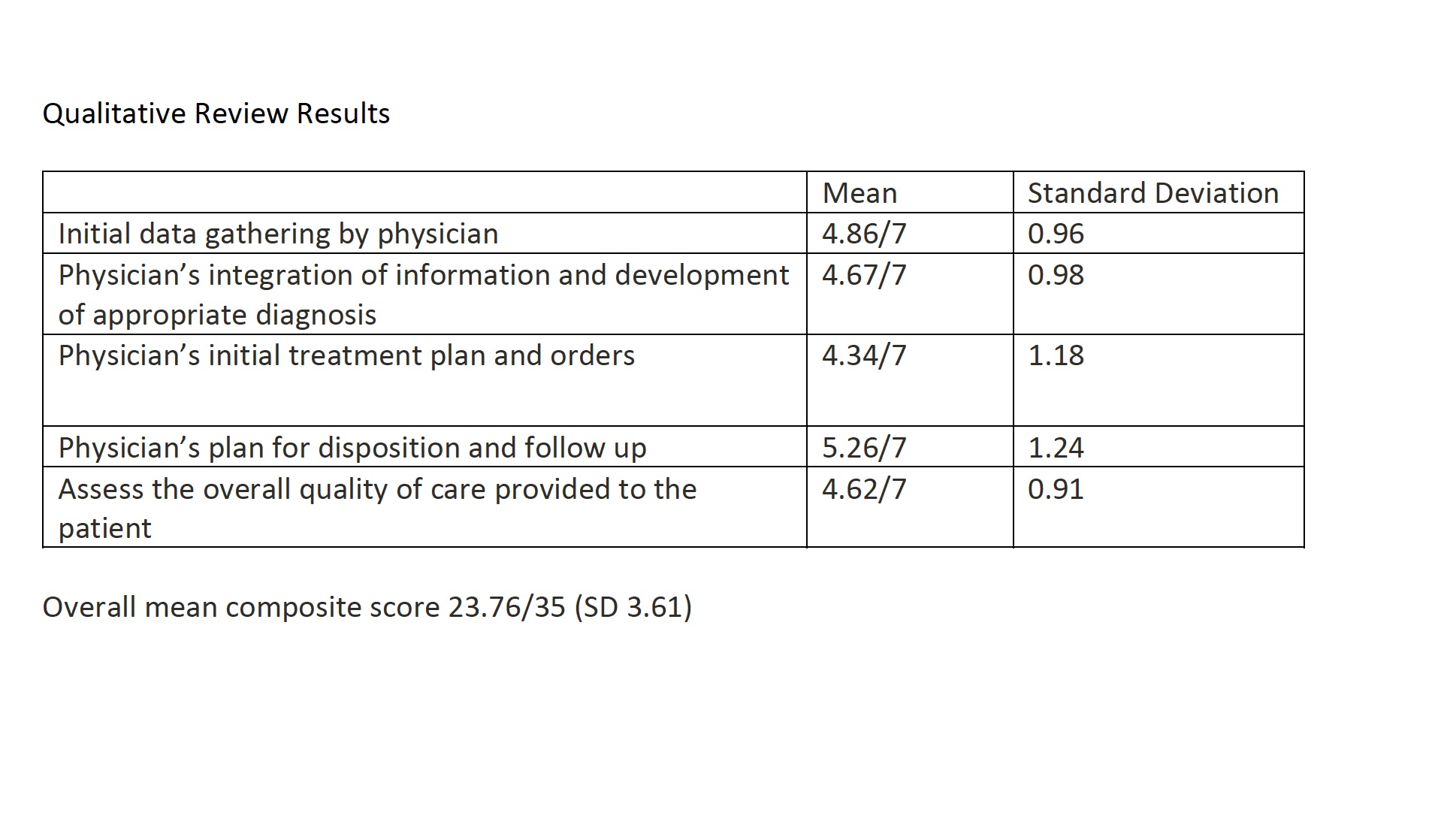
Results: 100 ESI level 2 and 1 ESI level 1 patients were reviewed. 82 charts were reviewed by 2 providers and 18 by 3. The average patient age was 6 (range < 1-17). Scores ranged from a low of 4.34 (SD 1.18) for initial treatment plan and orders to a high of 5.26 (SD 1.24) for plan for disposition and follow up. Results for each domain are summarized in the attached table. The overall mean composite score was 23.76/35 (SD 3.61)Conclusion(s): This review, while limited by its small size, raises concerns about the quality of care provided to pediatric patients seen in CAH ED. The low scores for development of appropriate diagnosis and for initial treatment plan and orders are concerning, CAH ED are staffed by providers with limited pediatric training and providers comfort level with the sickest children is likely limited. CAH ED would benefit from ongoing pediatric education. CAH ED would also benefit from access to telemedicine support from PEM trained physicians when caring for the sickest children. Qualitative Review Results