59 - Anemia, Iron Deficiency and FGF23 in CKiD Study
Sunday, April 24, 2022
3:30 PM – 6:00 PM US MT
Poster Number: 59 Publication Number: 59.341
Elizabeth Thomas, UCLA Mattel Childrens Hospital, Culver City, CA, United States; Marciana Laster, UCLA Mattel Childrens Hospital, Los Angeles, CA, United States; Susan Furth, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; BRADLEY A. WARADY, CHILDREN'S MERCY KANSAS CITY, KANSAS CITY, MO, United States; Alexandra M. Klomhaus, University of California, Los Angeles David Geffen School of Medicine, Los Angeles, CA, United States; Isidro B. Salusky, University of California, Los Angeles David Geffen School of Medicine, Los Angeles, CA, United States; Mark R. Hanudel, University of California, Los Angeles David Geffen School of Medicine, Los Angeles, CA, United States
Pediatric Nephrology Fellow UCLA Mattel Childrens Hospital Culver City, California, United States
Background: Fibroblast growth factor 23 (FGF23) is a bone-derived hormone fundamental to chronic kidney disease-mineral bone disorder (CKD-MBD), CKD progression, and CKD-associated cardiovascular morbidity. It has recently been demonstrated that non-mineral factors, such as iron deficiency and erythropoietin (EPO), can increase FGF23 production. CKD-associated anemia can be characterized by iron deficiency and/or compensatorily increased EPO levels.
Objective: The primary aims of this study are to assess whether anemia and/or iron deficiency are associated with increased FGF23 concentrations.
Design/Methods: Anemia, iron and FGF23 profiles were characterized in cross-sectional and longitudinal analyses of subjects enrolled in the CKiD study. Participants included children aged 1 month to 16 years old with mild to moderate CKD.
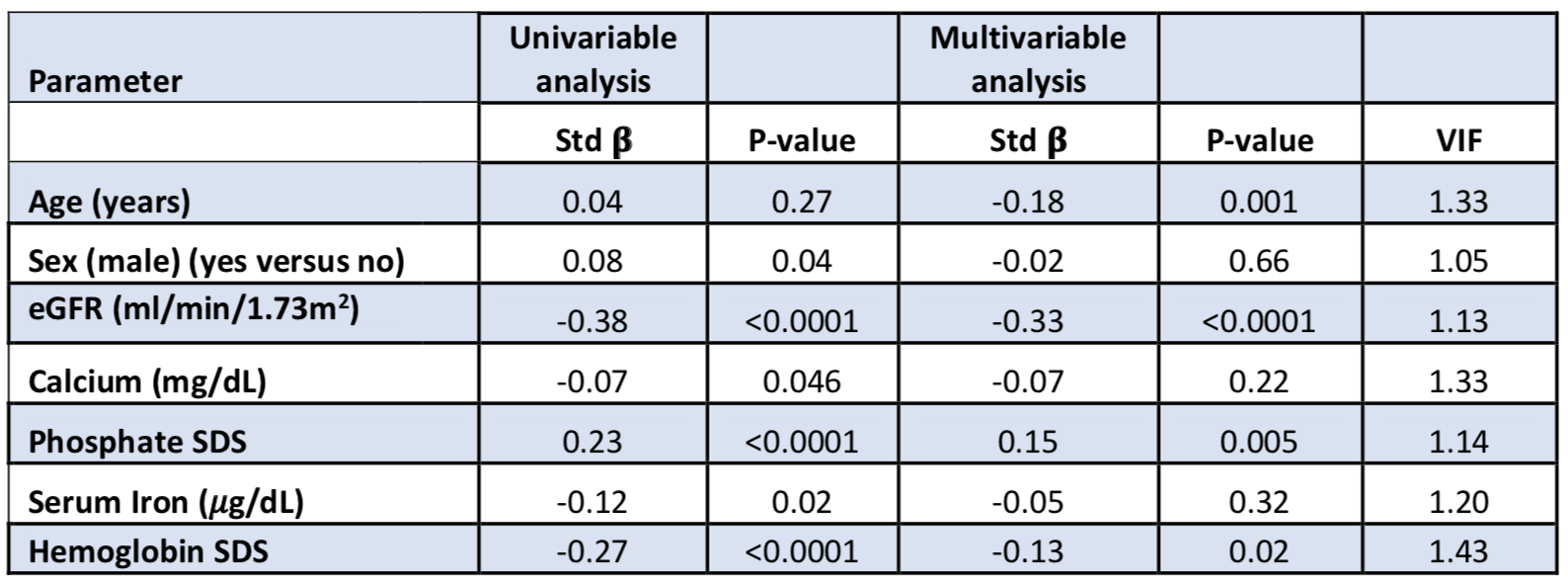
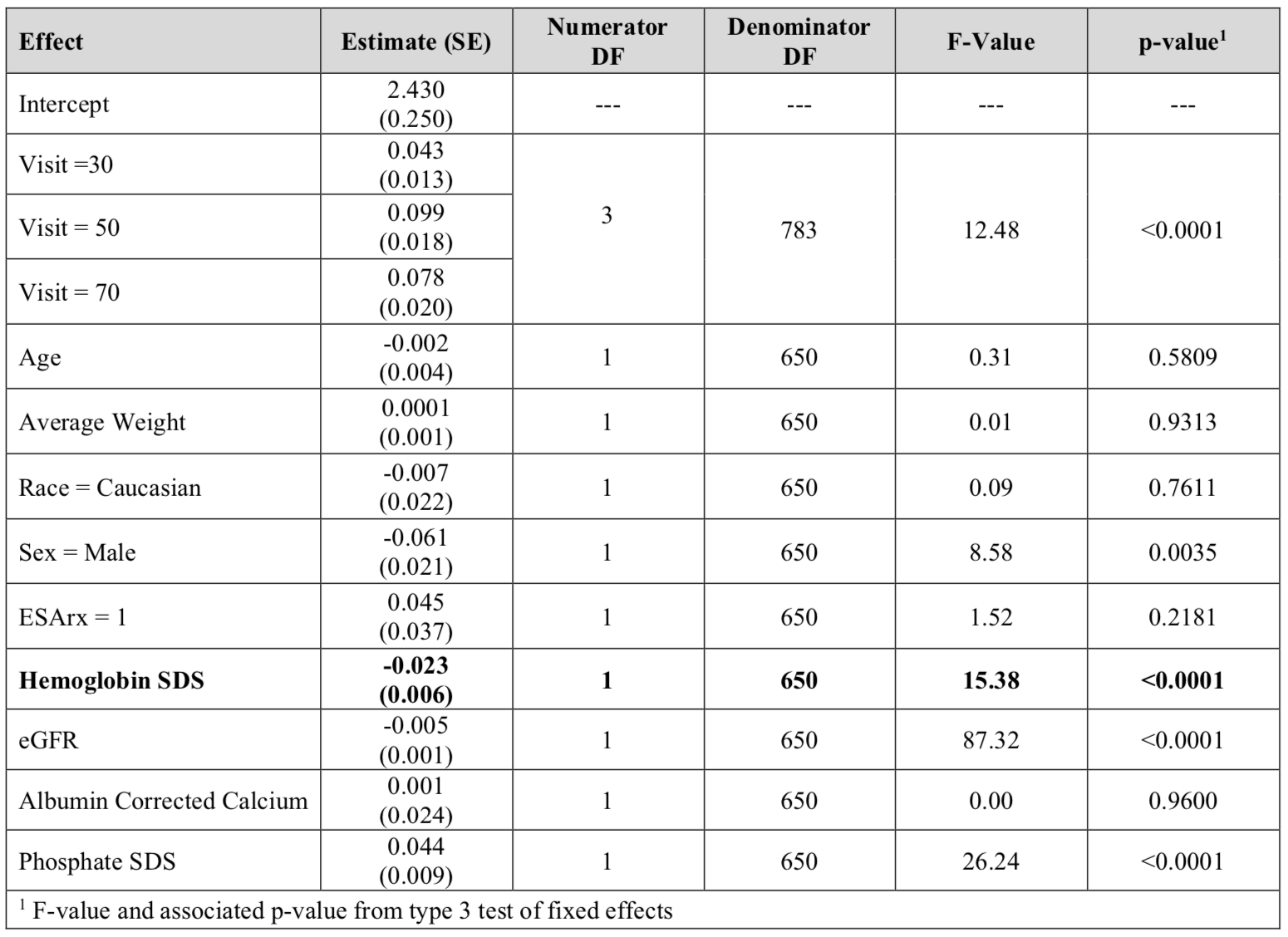
Results: In a cross-sectional analysis of 686 pediatric CKD patients at baseline (median (interquartile range) age 11 (8, 15) years, 62% male, 14% Hispanic), the median estimated glomerular filtration rate (eGFR) was 55 (41, 71) ml/min/1.73m2, and the median age-related hemoglobin standard deviation score (SDS) was -1.1 (-2.3, 0.2). Anemic subjects had higher C-terminal FGF23 SDS than non-anemic subjects (2.36 vs 1.01, p< 0.0001). In a multivariable linear regression model, log-transformed C-terminal FGF23 was independently and inversely associated with hemoglobin SDS (see Table 1). Log-transformed intact FGF23 was not significantly associated with hemoglobin SDS or serum iron. Change in hemoglobin SDS was additionally found to be inversely correlated to change in log-transformed C-terminal FGF23 over 2 years (Pearson correlation coefficient=-0.16, p=0.001). Using linear mixed effects models, longitudinal analyses over 6 years of follow up demonstrated that baseline hemoglobin SDS was inversely and independently associated with log-transformed C-terminal FGF23 (β =-0.023, p< 0.0001) (see Table 2). Likewise, baseline hemoglobin SDS had borderline significance with log-transformed intact FGF23 (β =-0.017, p=0.057).Conclusion(s): Decreased hemoglobin concentrations are independently associated with increased C-terminal FGF23 levels in pediatric CKD. This relationship is weaker with intact FGF23 levels, potentially implicating anemia-associated factors such as erythropoietin, increasing post-translational FGF23 cleavage. Further studies are warranted to identify and investigate these other influencing factors with FGF23. Table 1: Univariable and multivariable linear regression modeling of determinants of circulating log-transformed C-terminal FGF23 Table 2: Associations of baseline hemoglobin SDS with circulating log-transformed C-terminal FGF23 in a linear mixed effects model