Nephrology: Transplant
Category: Abstract Submission
Nephrology II: Transplant

Stella Kilduff, MD
Pediatric Nephrology Fellow
The Children's Hospital at Montefiore
Bronx, New York, United States
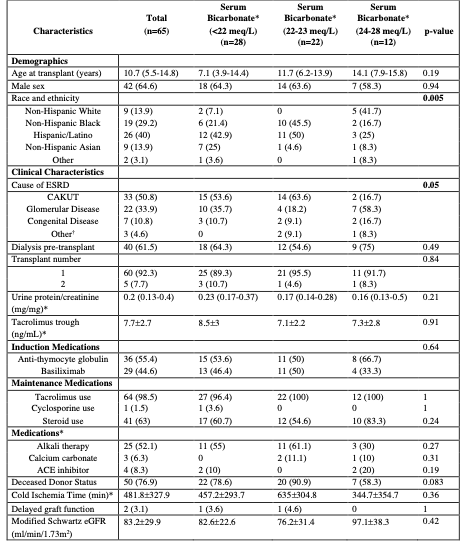 Abbreviations: ESRD=End Stage Renal Disease, CAKUT=Congenital Anomalies of the Kidneys & Urinary Tract, Alkali therapy= sodium bicarbonate/citrate/citric acid, ACE= Angiotensin-converting enzyme (ACE) inhibitors, eGFR= estimated Glomerular Filtration Rate.
Abbreviations: ESRD=End Stage Renal Disease, CAKUT=Congenital Anomalies of the Kidneys & Urinary Tract, Alkali therapy= sodium bicarbonate/citrate/citric acid, ACE= Angiotensin-converting enzyme (ACE) inhibitors, eGFR= estimated Glomerular Filtration Rate.