
Global Neonatal & Children's Health
Category: Abstract Submission
Global Child and Adolescent Health I

Ulrike Mietzsch, MD
Associate Professor of Clinical Pediatrics
University of Washington School of Medicine
Seattle, Washington, United States
.jpg) Admission characteristics of inborn infants admitted on the day of birth with a birth weight 2500 grams with a death or discharge diagnosis of asphyxia compared to a death or discharge diagnosis of infection.
Admission characteristics of inborn infants admitted on the day of birth with a birth weight 2500 grams with a death or discharge diagnosis of asphyxia compared to a death or discharge diagnosis of infection.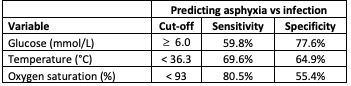 Optimal cut-offs for predicting asphyxia from individual admission variables, derived from 80% of infants with discharge or death diagnoses of infection or asphyxia.
Optimal cut-offs for predicting asphyxia from individual admission variables, derived from 80% of infants with discharge or death diagnoses of infection or asphyxia.