Neonatal Quality Improvement
Category: Abstract Submission
Neonatal Quality Improvement I

Dhruv Gupta, MD
Medical Director
Pediatrix
El Paso, Texas, United States
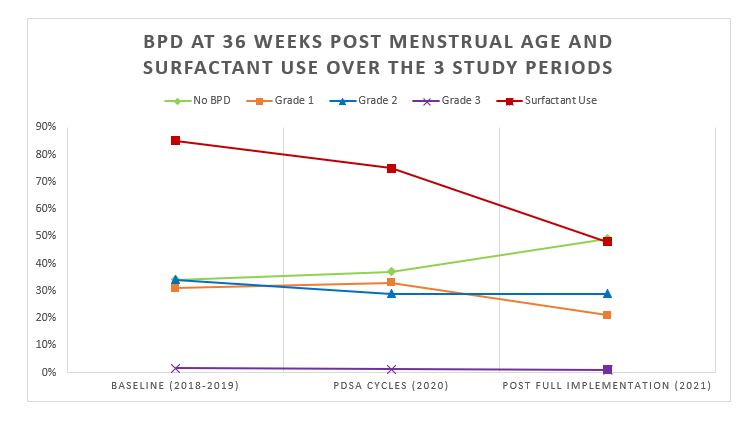
.jpg) Abbreviations: BPD: Bronchopulmonary dysplasia; NO BPD: no supplemental oxygen or flow; Grade 1 BPD: Nasal Cannula, Hood oxygen, Supplemental oxygen, Tracheal oxygen; Grade 2 BPD: Endotracheal continuous positive airway pressure, High flow nasal cannula, Nasal prong ventilation, Nasal continuous positive airway pressure, Tracheal continuous positive airway pressure; Grade 3 BPD: Ventilator, Jet Ventilator, Oscillator
Abbreviations: BPD: Bronchopulmonary dysplasia; NO BPD: no supplemental oxygen or flow; Grade 1 BPD: Nasal Cannula, Hood oxygen, Supplemental oxygen, Tracheal oxygen; Grade 2 BPD: Endotracheal continuous positive airway pressure, High flow nasal cannula, Nasal prong ventilation, Nasal continuous positive airway pressure, Tracheal continuous positive airway pressure; Grade 3 BPD: Ventilator, Jet Ventilator, Oscillator