
Critical Care
Category: Abstract Submission
Critical Care I
Shyam J. Deshpande, MD, FAAP
Resident in Anesthesiology & Pain Medicine
University of Washington School of Medicine
Seattle, Washington, United States
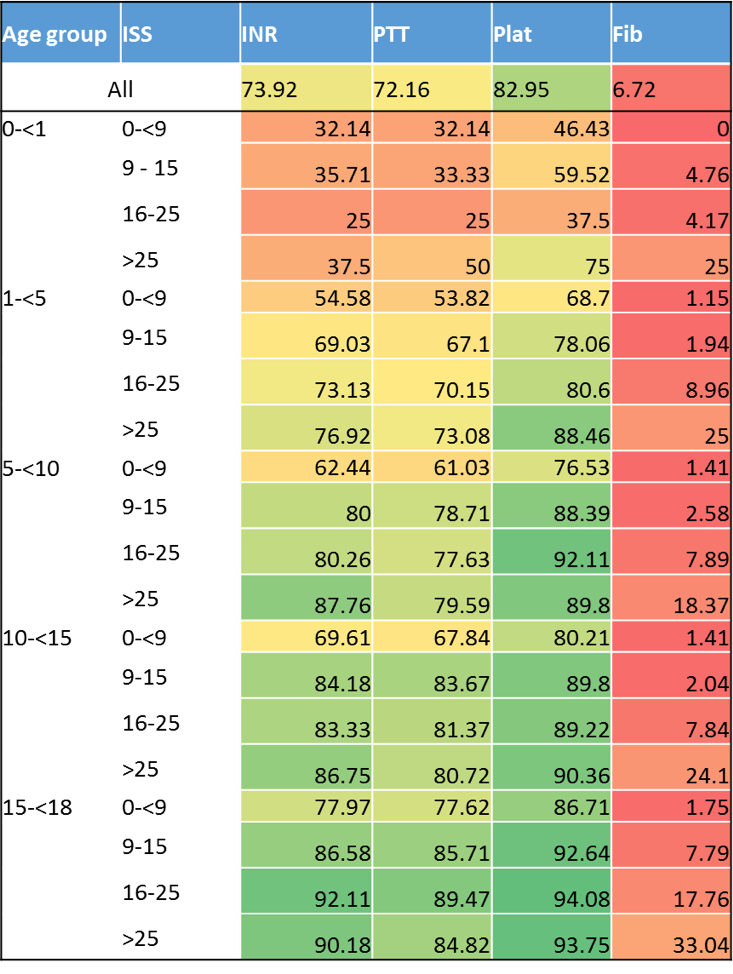 Laboratory study data availability at the time of trauma admission by age group and ISS group, demonstrating the relative infrequency of study acquisition in the youngest age group, as well as the paucity of fibrinogen values obtain. Cell color fill scaled by percentage, with green cells representing the highest data availability and red cells representing the lowest data availability.
Laboratory study data availability at the time of trauma admission by age group and ISS group, demonstrating the relative infrequency of study acquisition in the youngest age group, as well as the paucity of fibrinogen values obtain. Cell color fill scaled by percentage, with green cells representing the highest data availability and red cells representing the lowest data availability.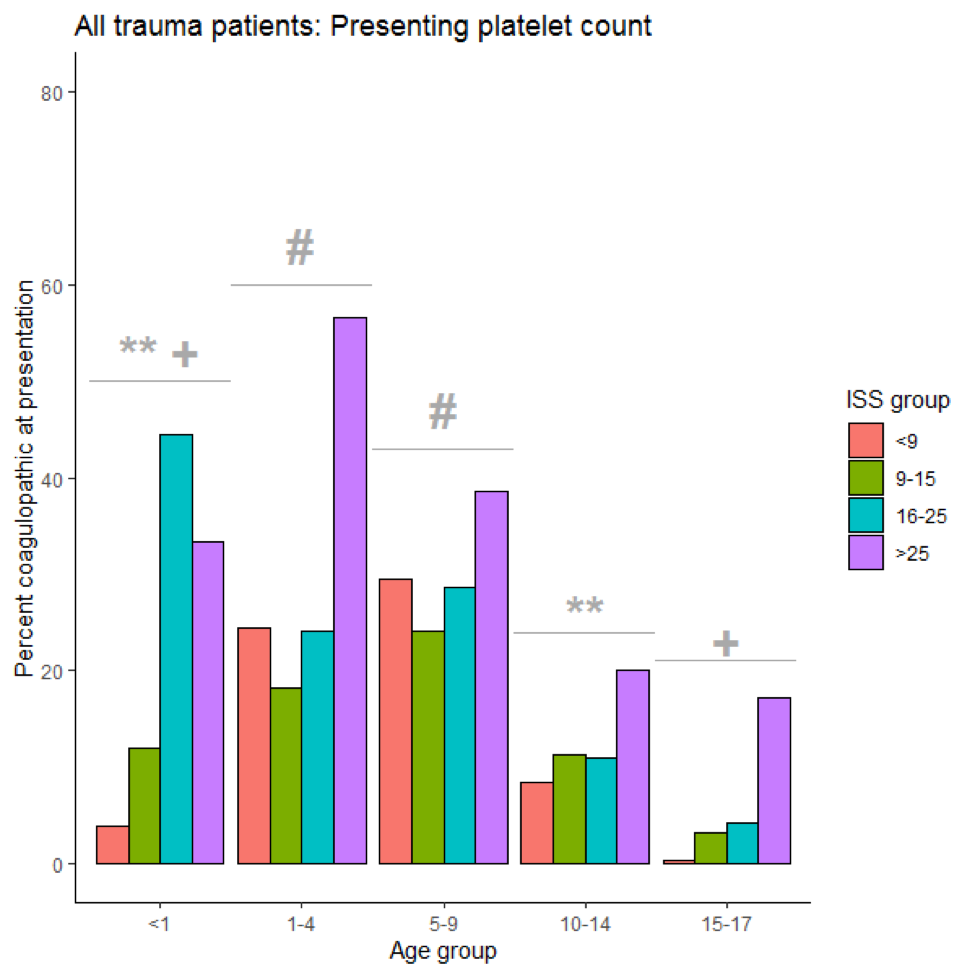 Frequency of coagulopathy defined by platelet count below age-specific reference ranges at the time of trauma admission by pediatric age group and ISS group, demonstrating higher frequency of coagulopathy in younger children compared to older children. Symbols above age groups represent statistically unique groups in frequency of coagulopathy (eg. frequency of coagulopathy for 1-4 is statistically higher than < 1y, 10-14y, and 15-17y and not statistically different from 5-9y).
Frequency of coagulopathy defined by platelet count below age-specific reference ranges at the time of trauma admission by pediatric age group and ISS group, demonstrating higher frequency of coagulopathy in younger children compared to older children. Symbols above age groups represent statistically unique groups in frequency of coagulopathy (eg. frequency of coagulopathy for 1-4 is statistically higher than < 1y, 10-14y, and 15-17y and not statistically different from 5-9y).