
Infectious Diseases
Category: Abstract Submission
Infectious Diseases: Bacteria & Antimicrobials
Priya K. Patel, MD
All Children’s Hospital Foundation grant
St. Petersburg, Florida, United States
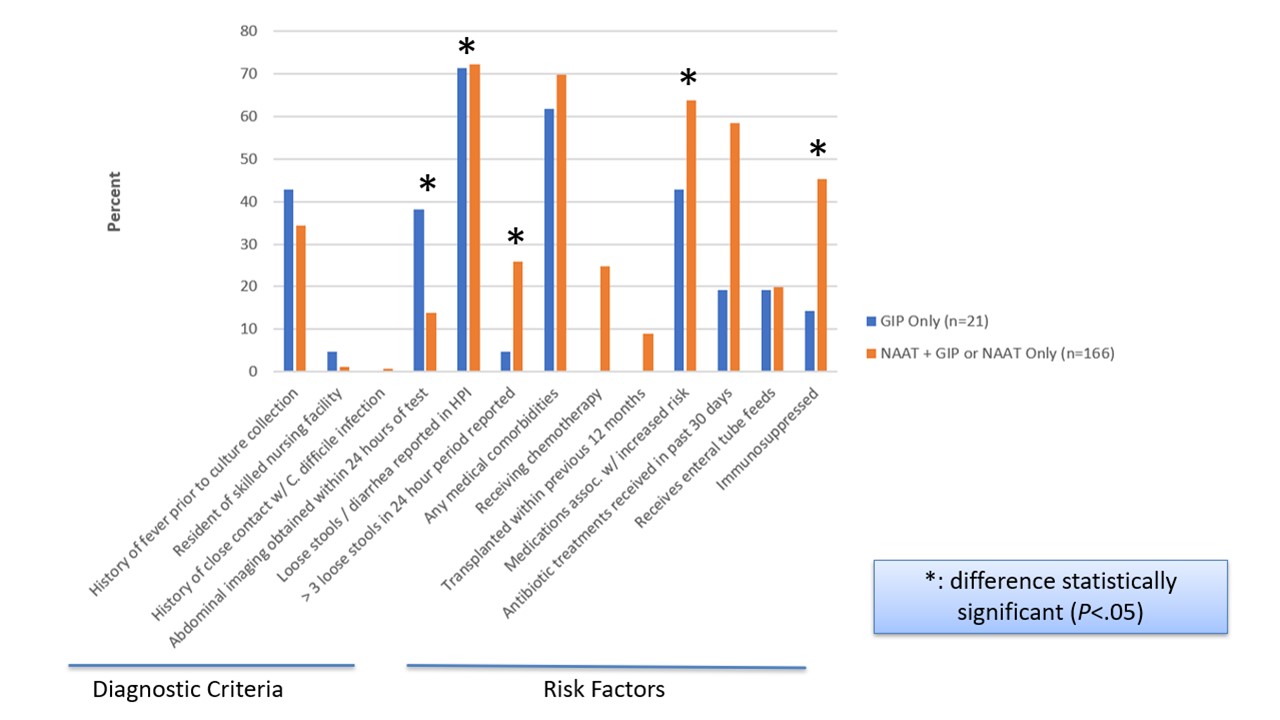 Diagnostic criteria and risk factors for C. difficile infection by targeted C. difficile test status
Diagnostic criteria and risk factors for C. difficile infection by targeted C. difficile test status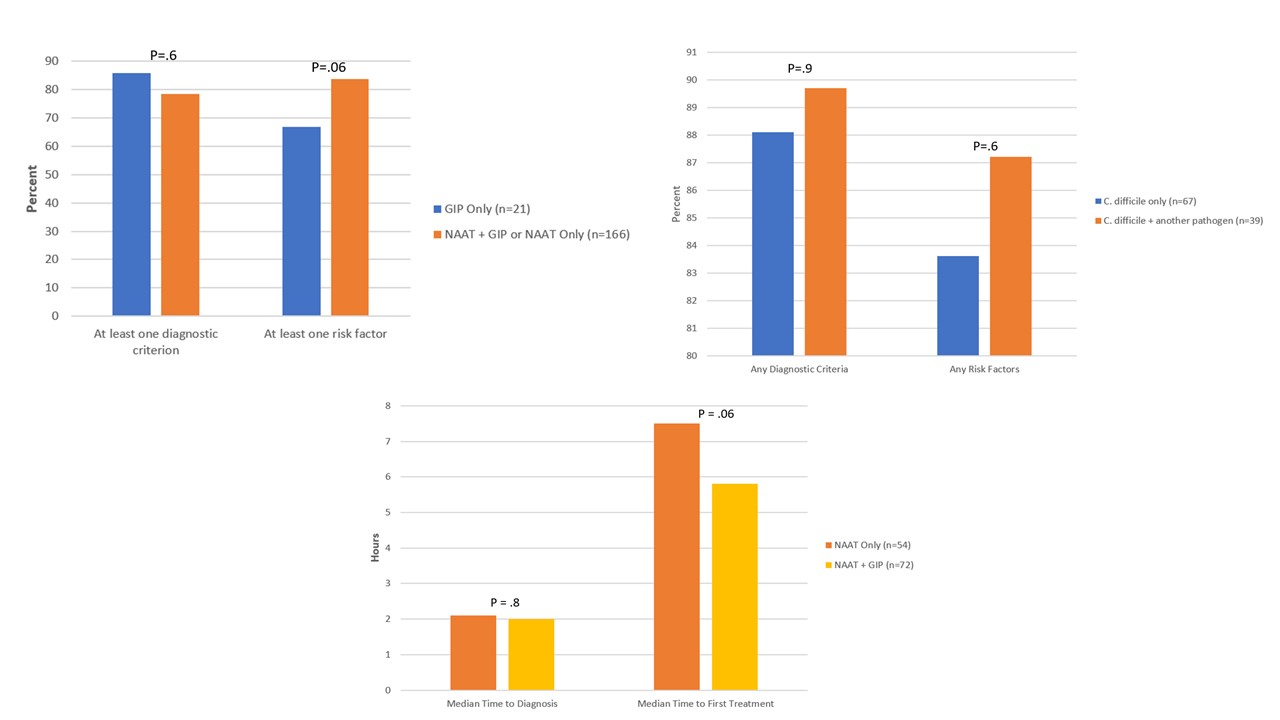 Diagnostic criteria and risk factors for C. difficile infection by targeted C. difficile test status; Diagnostic criteria and risk factors for C. difficile infection by coinfection status among patients with NAAT+GIP or GIP testing only; Time to diagnosis and treatment among patients treated for C. difficile infection by type of C. difficile test
Diagnostic criteria and risk factors for C. difficile infection by targeted C. difficile test status; Diagnostic criteria and risk factors for C. difficile infection by coinfection status among patients with NAAT+GIP or GIP testing only; Time to diagnosis and treatment among patients treated for C. difficile infection by type of C. difficile test