
Neonatal Quality Improvement
Category: Abstract Submission
Neonatal Quality Improvement I
Rishika P. Sakaria, MD (she/her/hers)
Assistant Professor
University of Tennessee Health Science Center College of Medicine
The University of Tennessee Health Science Center
Memphis, Tennessee, United States
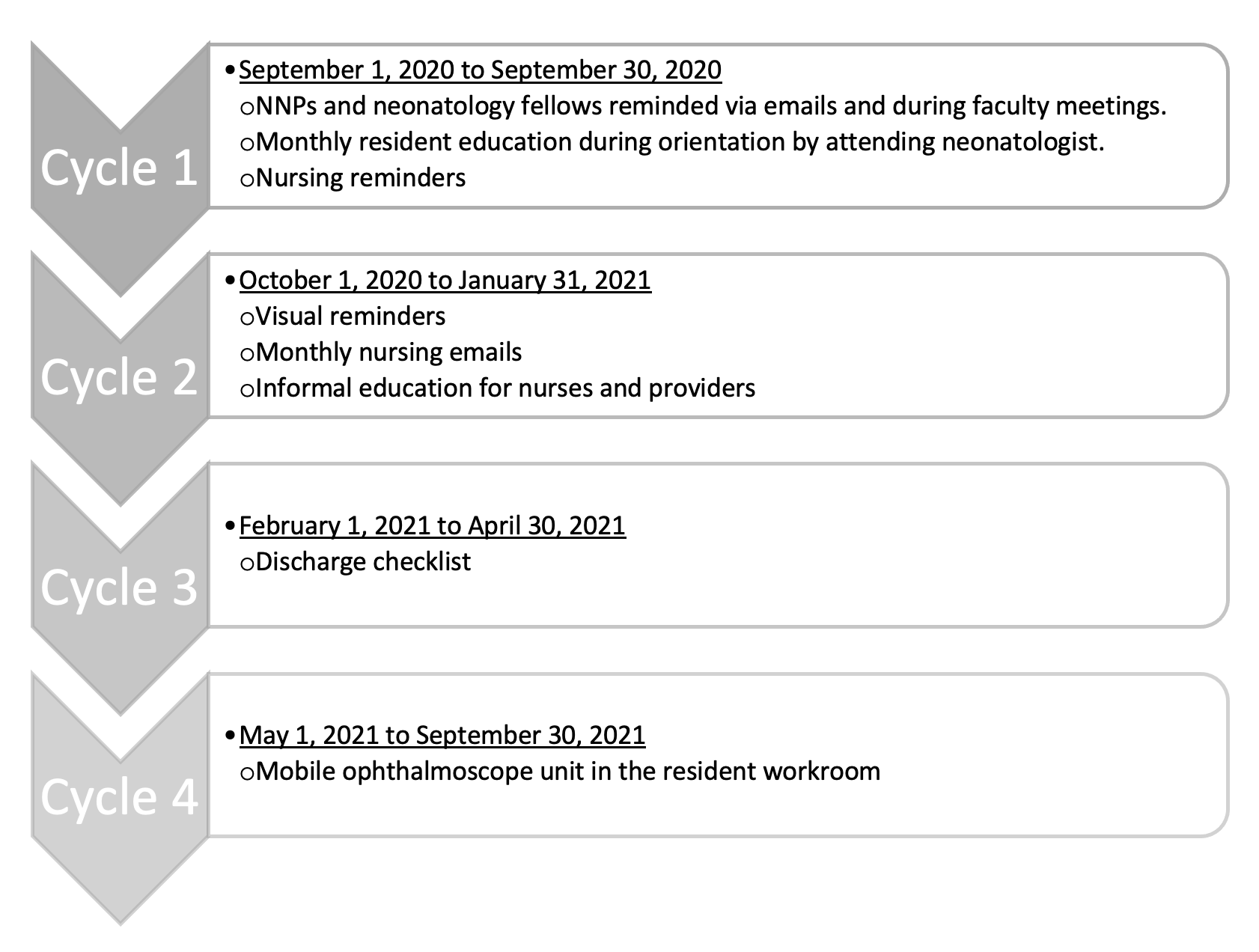 PDSA cycles implemented to achieve SMART aim
PDSA cycles implemented to achieve SMART aim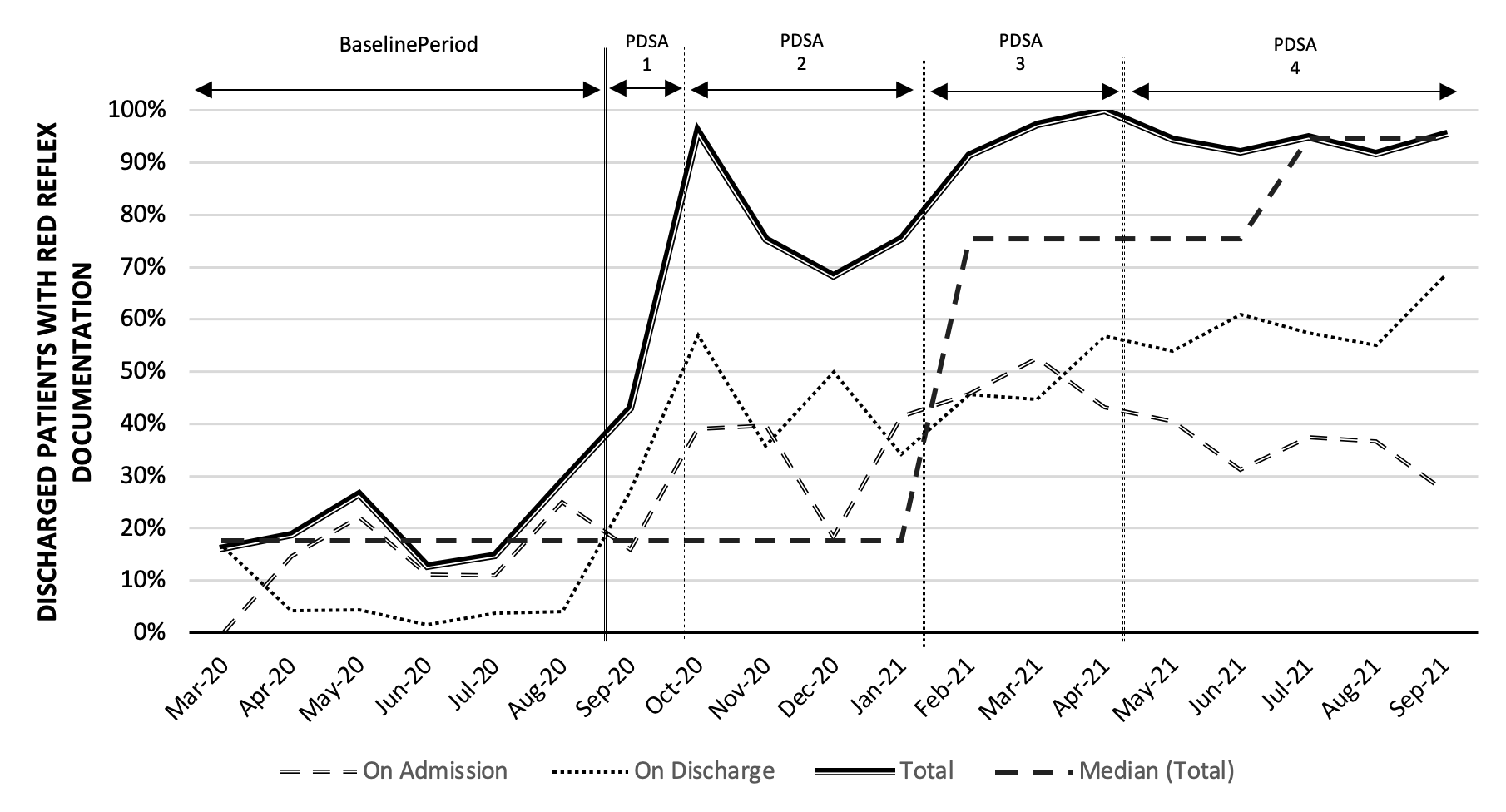 Overall trends in the red reflex documentation rate during the project period during various PDSA cycles. There was a significant positive shift in the median from 17.55% to 75.4% during the intervention period during PDSA cycle 3 and further to 94.5% during PDSA cycle 4.
Overall trends in the red reflex documentation rate during the project period during various PDSA cycles. There was a significant positive shift in the median from 17.55% to 75.4% during the intervention period during PDSA cycle 3 and further to 94.5% during PDSA cycle 4.