
Emergency Medicine: All Areas
Category: Abstract Submission
Emergency Medicine III

Quinney Fu, MD
Pediatric Emergency Medicine Fellow
Phoenix Children's
Phoenix, Arizona, United States
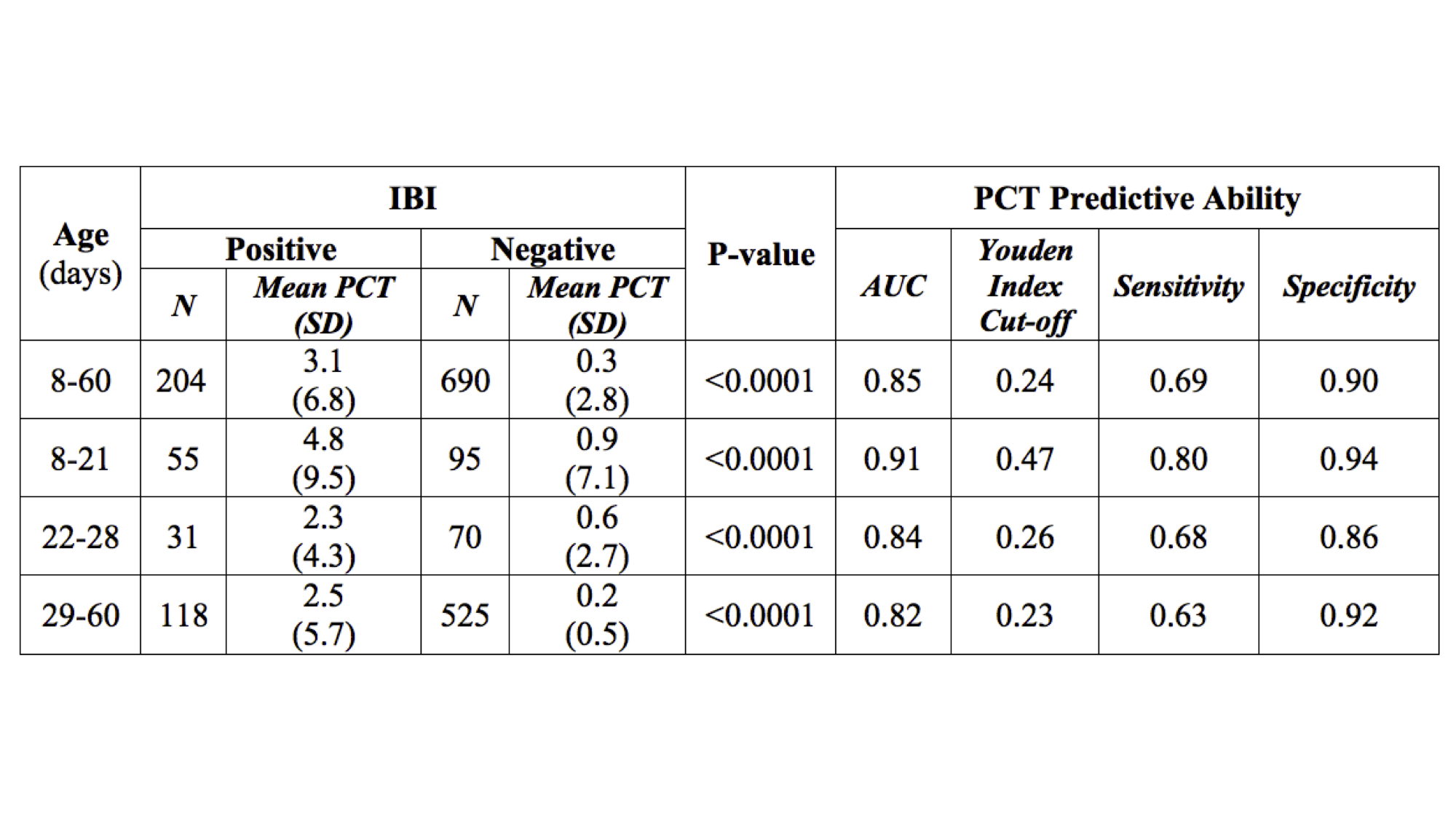 PCT and IBI in febrile infants ages 8-60 days. PCT= Procalcitonin; IBI= Invasive bacterial infection; SD= Standard deviation; AUC= Area under the curve.
PCT and IBI in febrile infants ages 8-60 days. PCT= Procalcitonin; IBI= Invasive bacterial infection; SD= Standard deviation; AUC= Area under the curve.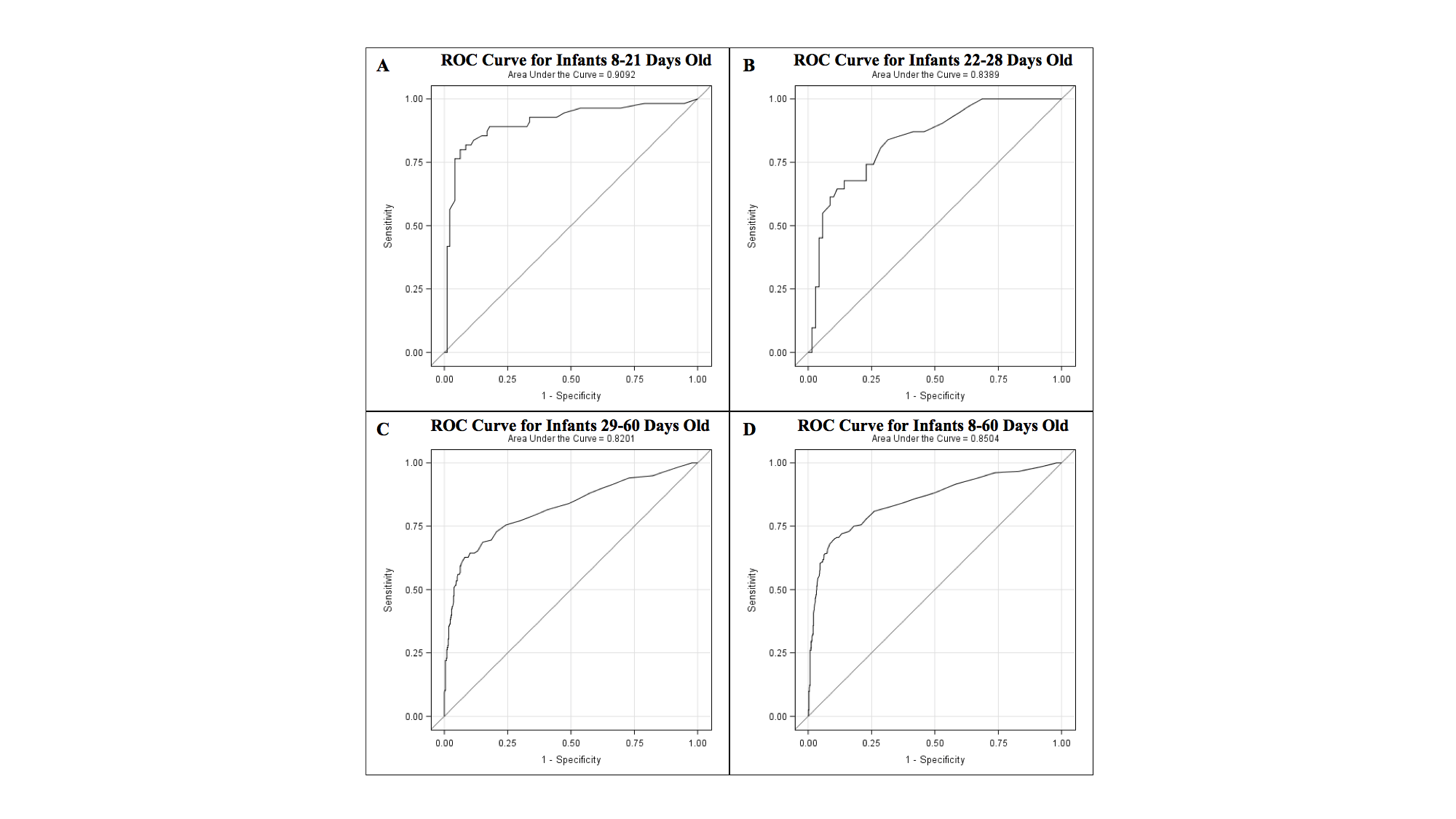 The ROC curves of PCT for febrile infants A. 8-21 days old, B. 22-28 days old, C. 29-60 days old, and D. 8-60 days old for the diagnosis of IBI. ROC= Receiver operating characteristics; PCT= Procalcitonin; IBI= Invasive bacterial infection.
The ROC curves of PCT for febrile infants A. 8-21 days old, B. 22-28 days old, C. 29-60 days old, and D. 8-60 days old for the diagnosis of IBI. ROC= Receiver operating characteristics; PCT= Procalcitonin; IBI= Invasive bacterial infection.