
Neonatal Infectious Diseases/Immunology
Category: Abstract Submission
Neonatal Infectious Diseases/Immunology: COVID-19
Kristen Smith, MD
Neonatal-Perinatal Fellow
Walter Reed National Military Medical Center
Bethesda, Maryland, United States
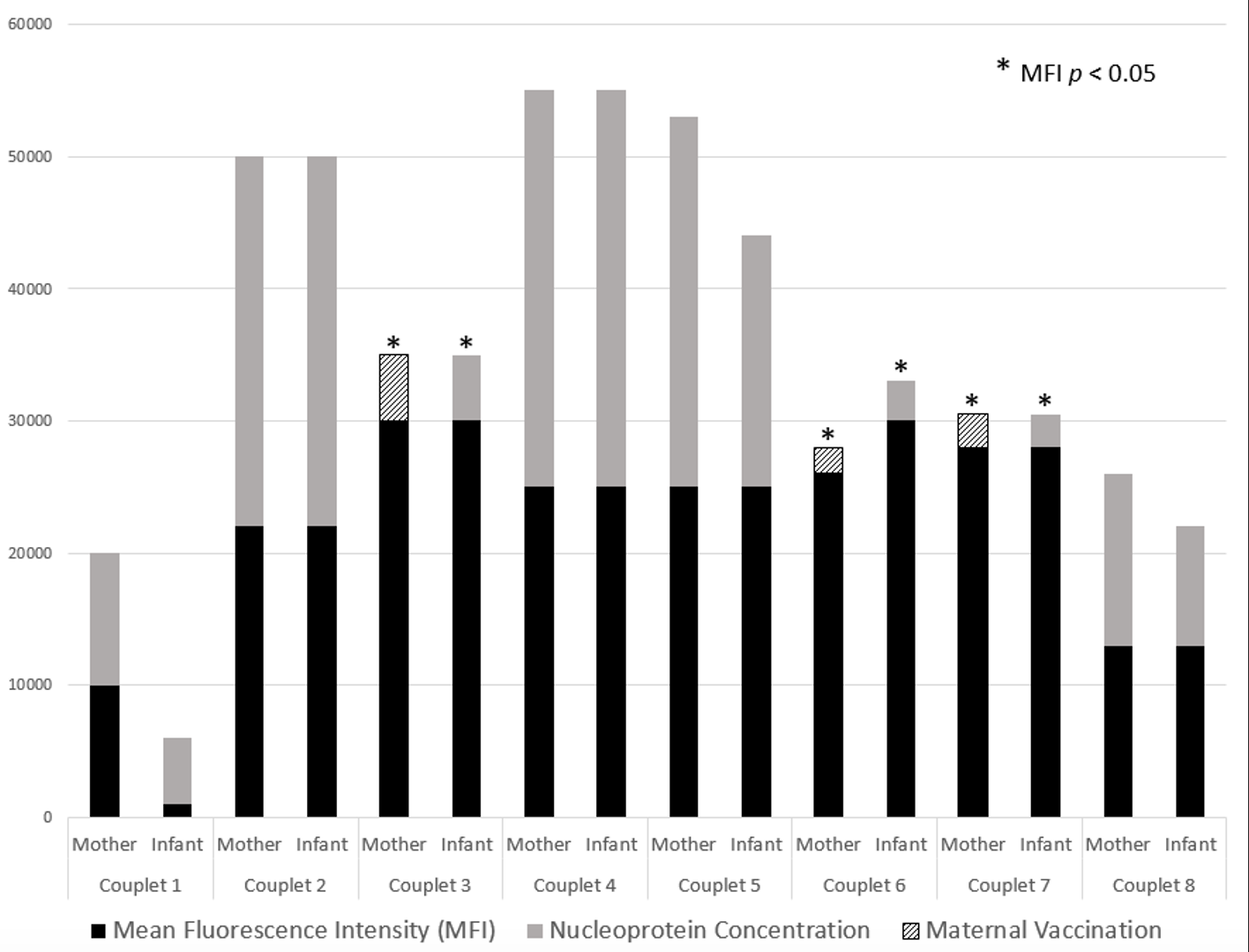 SARS-CoV-2 IgG concentrations present in maternal and fetal circulation represented by mean fluorescence intensity (MFI). Native maternal infection confirmed via SARS-CoV-2 nucleoprotein presence in maternal serum and infant cord blood. A statistically significant association was found in the MFI of mothers who experienced both infection and immunization during their pregnancy (p = 0.04) and this correlated with a statistically significant MFI in their respective offspring (p = 0.04). There was no statistical significance in unimmunized, but previously infected, mothers or their offspring.
SARS-CoV-2 IgG concentrations present in maternal and fetal circulation represented by mean fluorescence intensity (MFI). Native maternal infection confirmed via SARS-CoV-2 nucleoprotein presence in maternal serum and infant cord blood. A statistically significant association was found in the MFI of mothers who experienced both infection and immunization during their pregnancy (p = 0.04) and this correlated with a statistically significant MFI in their respective offspring (p = 0.04). There was no statistical significance in unimmunized, but previously infected, mothers or their offspring.