
Neonatal Clinical Trials
Category: Abstract Submission
Neonatal Clinical Trials I

William E. King, MSEE
CEO
Medical Predictive Science Corporation
Charlottesville, Virginia, United States
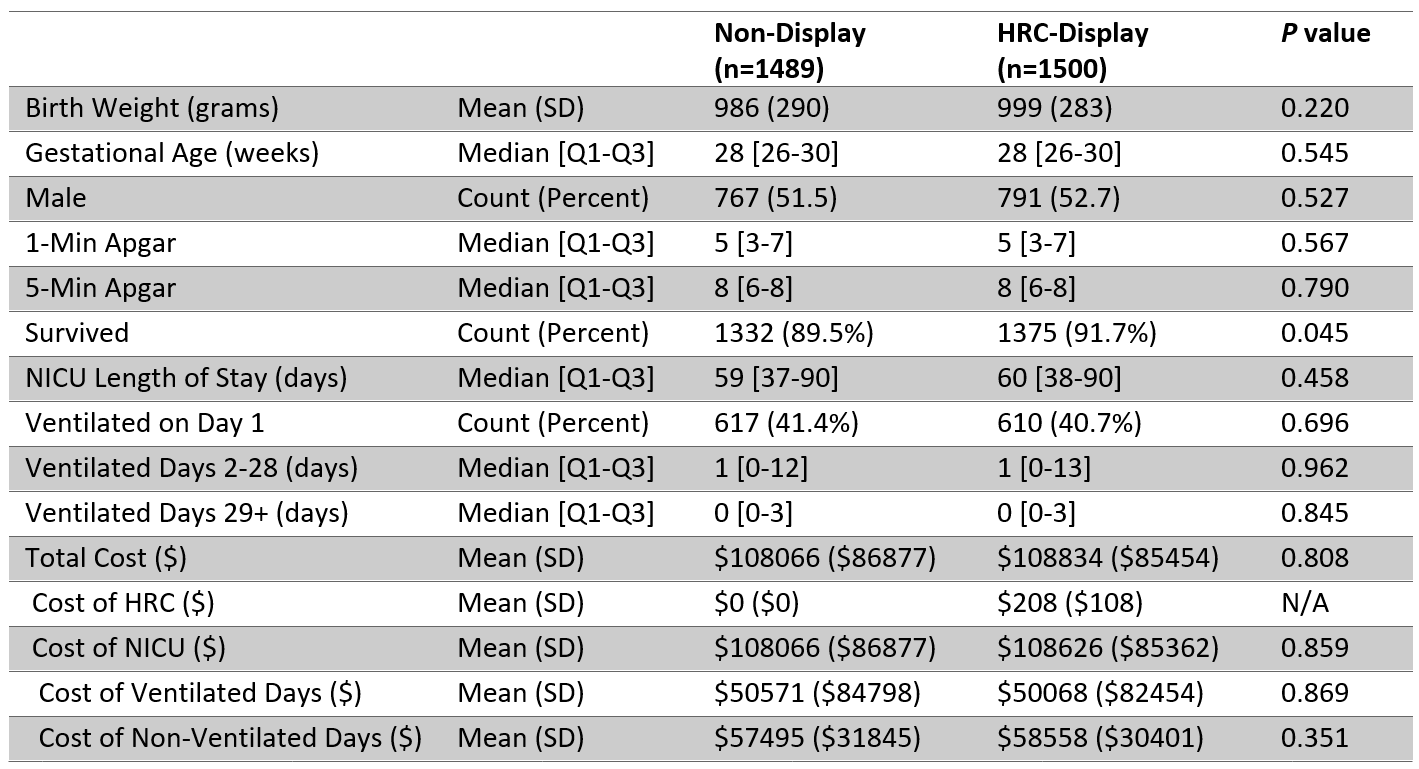 Demographics, Mortality, and Resource Utilization by Randomization Arm. A 2-sided t test is used to assess the significance of continuous variables, a Wilcoxon rank-sum test for ordinal variables, and a test for equality of proportions for categorical variables.
Demographics, Mortality, and Resource Utilization by Randomization Arm. A 2-sided t test is used to assess the significance of continuous variables, a Wilcoxon rank-sum test for ordinal variables, and a test for equality of proportions for categorical variables.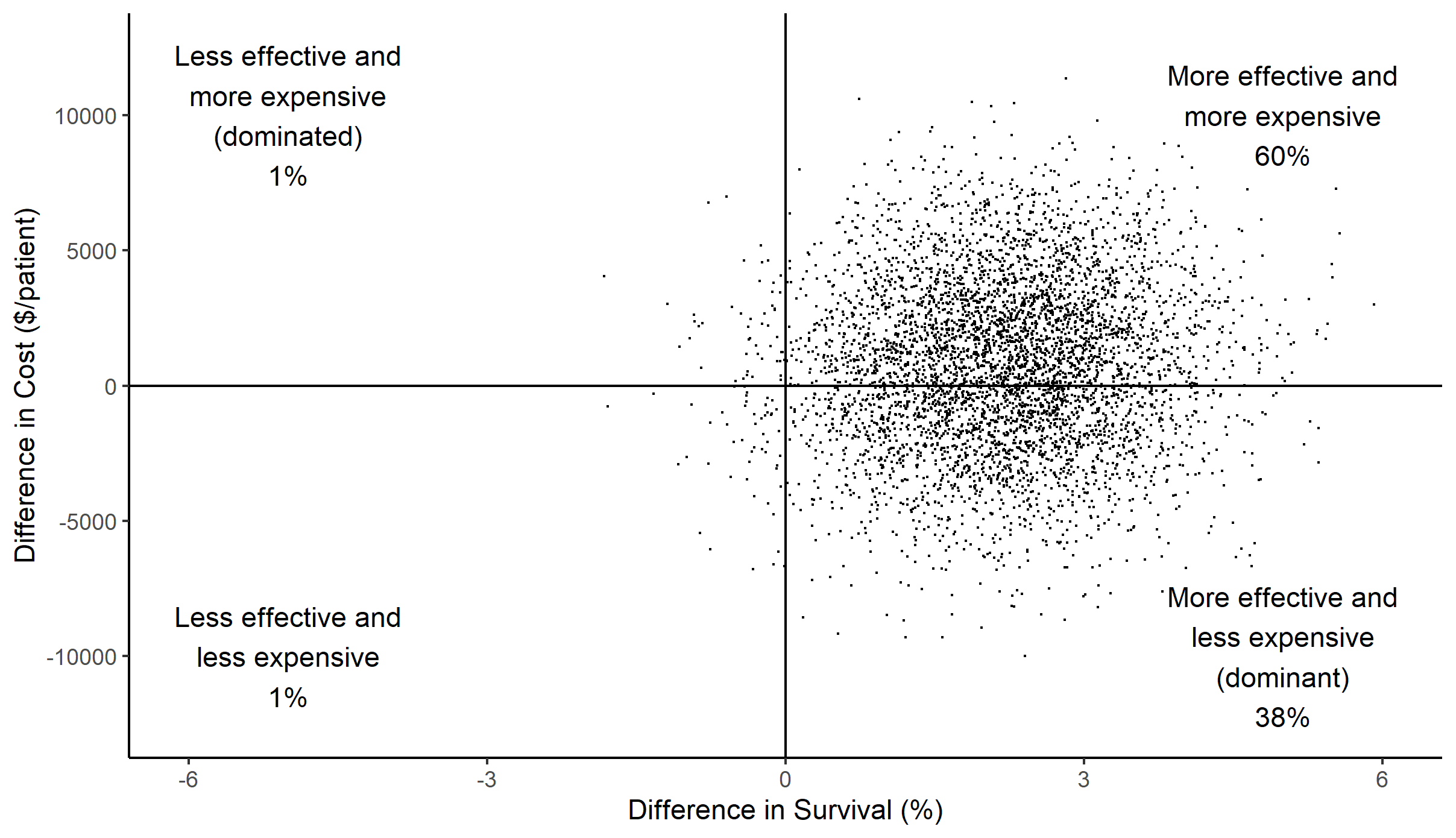 Scatterplot of difference in cost versus difference in effect (survival) between HRC-display and non-display arms for each of 5000 simulations. A large majority of points fall in the right half of the graph, indicating that HRC-monitoring was effective at reducing mortality; the smaller majority of data in the top half indicates that differences in cost were modest.
Scatterplot of difference in cost versus difference in effect (survival) between HRC-display and non-display arms for each of 5000 simulations. A large majority of points fall in the right half of the graph, indicating that HRC-monitoring was effective at reducing mortality; the smaller majority of data in the top half indicates that differences in cost were modest.