
Neonatal General
Category: Abstract Submission
Neonatology General 8: Health Disparities - Health Services Research
 photo")
Brynne A. Sullivan, MD, MSCR (she/her/hers)
Assistant Professor
University of Virginia
Charlottesville, Virginia, United States
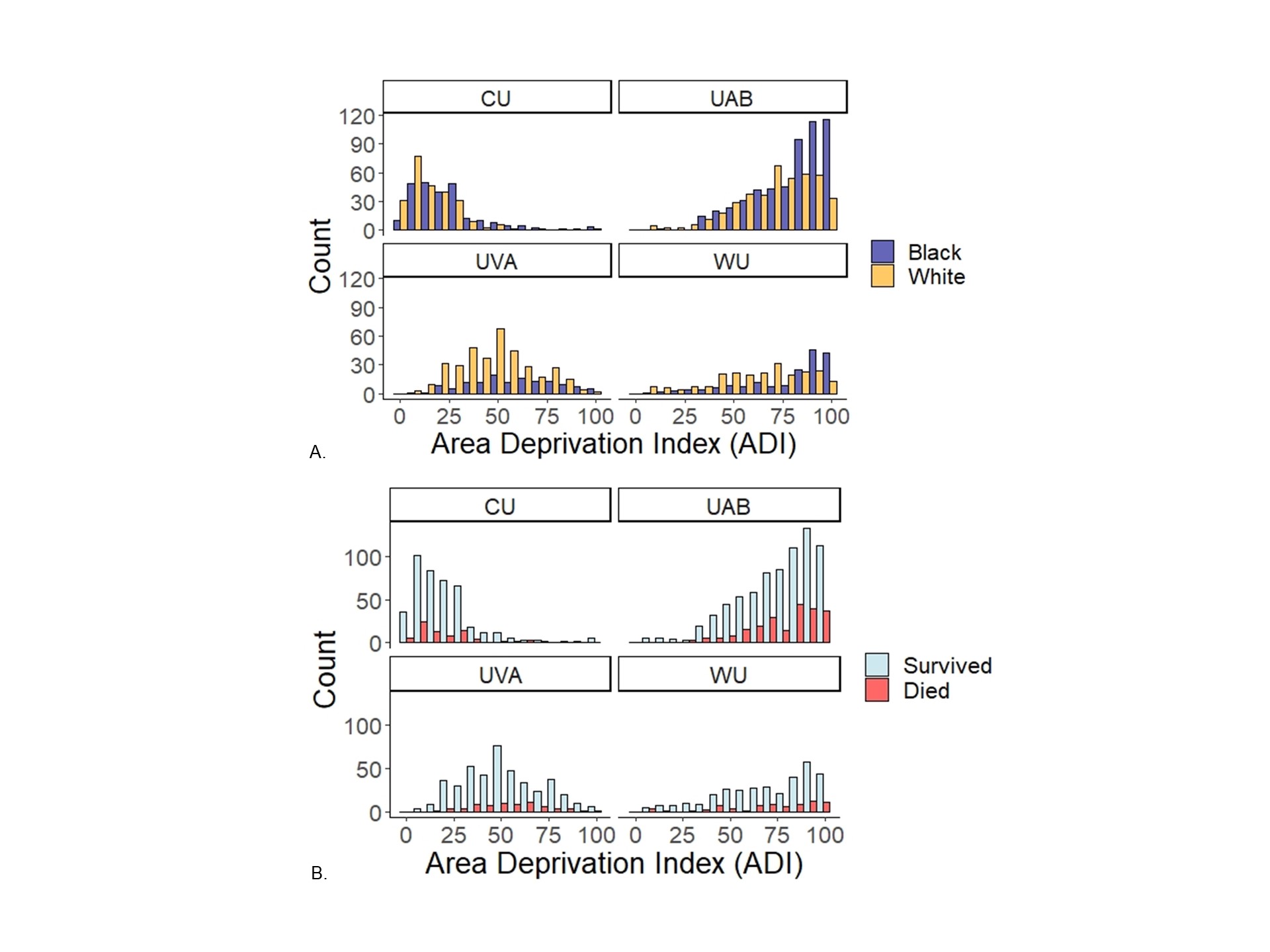 National ranked Area Deprivation Index percentiles in infants < 29 weeks gestational age at four NICUs. Panel A compares ADI between Black and White infants and Panel B compares ADI between survivors and non-survivors. ADI distributions were similar by survival status at each site but differed by race at each site, with higher ADI percentiles in Black infants compared to White. UVA = University of Virginia, WU = Washington University in St. Louis, CU = Columbia University, UAB = University of Alabama
National ranked Area Deprivation Index percentiles in infants < 29 weeks gestational age at four NICUs. Panel A compares ADI between Black and White infants and Panel B compares ADI between survivors and non-survivors. ADI distributions were similar by survival status at each site but differed by race at each site, with higher ADI percentiles in Black infants compared to White. UVA = University of Virginia, WU = Washington University in St. Louis, CU = Columbia University, UAB = University of Alabama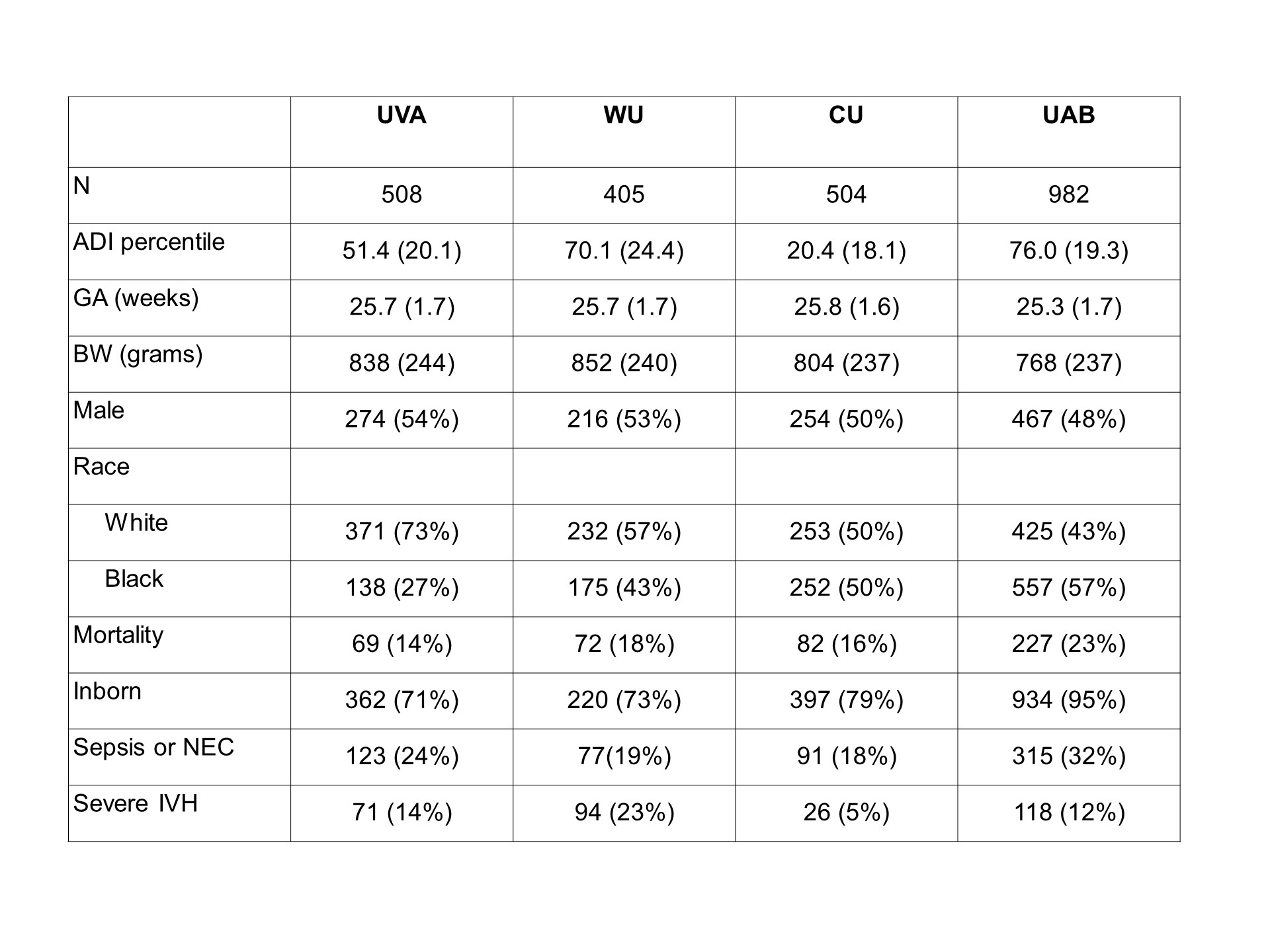 Variables are presented as mean (SD) or number (%). UVA = University of Virginia, WU = Washington University in St. Louis, CU = Columbia University, UAB = University of Alabama, NEC = necrotizing enterocolitis, Bell’s stage 2-3, Severe IVH = grade 3-4 intraventricular hemorrhage
Variables are presented as mean (SD) or number (%). UVA = University of Virginia, WU = Washington University in St. Louis, CU = Columbia University, UAB = University of Alabama, NEC = necrotizing enterocolitis, Bell’s stage 2-3, Severe IVH = grade 3-4 intraventricular hemorrhage