
Breastfeeding/Human Milk
Category: Abstract Submission
Breastfeeding/Human Milk II

Margaret L. Ong, MD
Clinical Fellow
Boston Children's Hospital
Boston, Massachusetts, United States
.jpg) Data are expressed as mean ± SD or n (%). Z-scores for anthropometric measurements are based on Fenton 2013. Global brain abnormality scores are based on Kidokoro 2013. NEC: necrotizing enterocolitis. FA: fractional anisotropy. PLIC: posterior limb of the internal capsule. CC: corpus callosum.
Data are expressed as mean ± SD or n (%). Z-scores for anthropometric measurements are based on Fenton 2013. Global brain abnormality scores are based on Kidokoro 2013. NEC: necrotizing enterocolitis. FA: fractional anisotropy. PLIC: posterior limb of the internal capsule. CC: corpus callosum.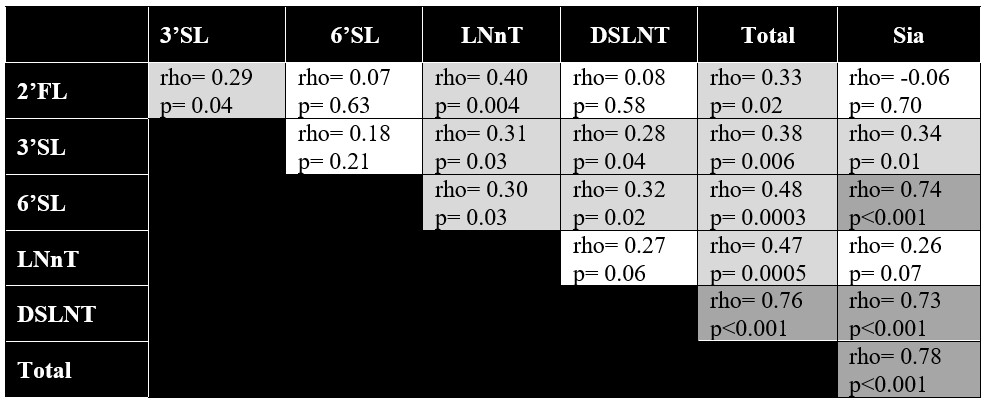 Mean area under the curve for concentrations of specific and total HMOs and HMO-bound sialic acid were analyzed using Spearman’s correlation. Box colors represent strength of correlation, with darker gray depicting stronger correlations. 2’FL: 2’fucosyllactose. 3’SL: 3’sialyllactose. 6’SL: 6’sialyllactose. LNnT: lacto-N-neotetraose. DSLNT: disialyllacto-N-tetraose. Sia: HMO-bound sialic acid.
Mean area under the curve for concentrations of specific and total HMOs and HMO-bound sialic acid were analyzed using Spearman’s correlation. Box colors represent strength of correlation, with darker gray depicting stronger correlations. 2’FL: 2’fucosyllactose. 3’SL: 3’sialyllactose. 6’SL: 6’sialyllactose. LNnT: lacto-N-neotetraose. DSLNT: disialyllacto-N-tetraose. Sia: HMO-bound sialic acid.