
Neonatal GI Physiology & NEC
Category: Abstract Submission
Neonatal GI Physiology & NEC III
 photo")
Shruti Patel, MD (she/her/hers)
Neonatology Fellow
University of Maryland School of Medicine
Baltimore, Maryland, United States
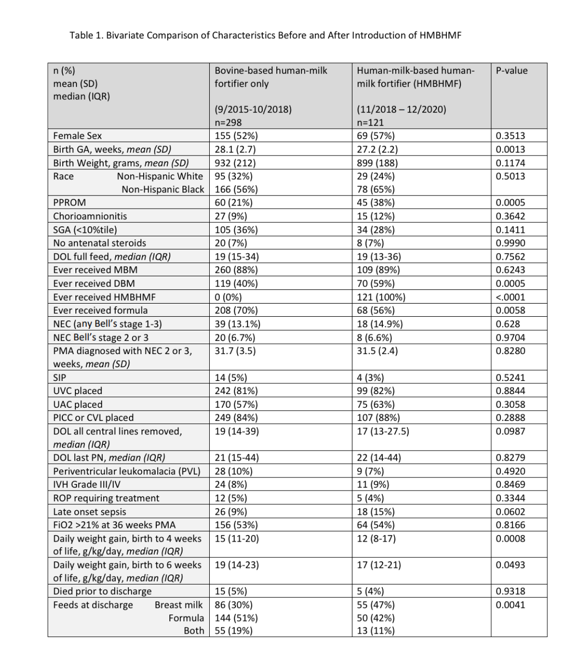 CVL, central venous line surgically placed; DBM, donor breast milk; DOL, day of life; GA, gestational age; HMBHMF, human-milk-based human-milk fortifier; IVH, intraventricular hemorrhage; MBM, maternal breast milk; NEC, necrotizing enterocolitis; PICC, peripherally inserted central catheter; PMA, post-menstrual age in weeks; PN, parenteral nutrition; PPROM, prolonged premature rupture of membranes; ROP, retinopathy of prematurity; SGA, small for gestational age status < 10%tile; SIP, spontaneous intestinal perforation; UAC, umbilical arterial catheter; UVC, umbilical venous catheter
CVL, central venous line surgically placed; DBM, donor breast milk; DOL, day of life; GA, gestational age; HMBHMF, human-milk-based human-milk fortifier; IVH, intraventricular hemorrhage; MBM, maternal breast milk; NEC, necrotizing enterocolitis; PICC, peripherally inserted central catheter; PMA, post-menstrual age in weeks; PN, parenteral nutrition; PPROM, prolonged premature rupture of membranes; ROP, retinopathy of prematurity; SGA, small for gestational age status < 10%tile; SIP, spontaneous intestinal perforation; UAC, umbilical arterial catheter; UVC, umbilical venous catheter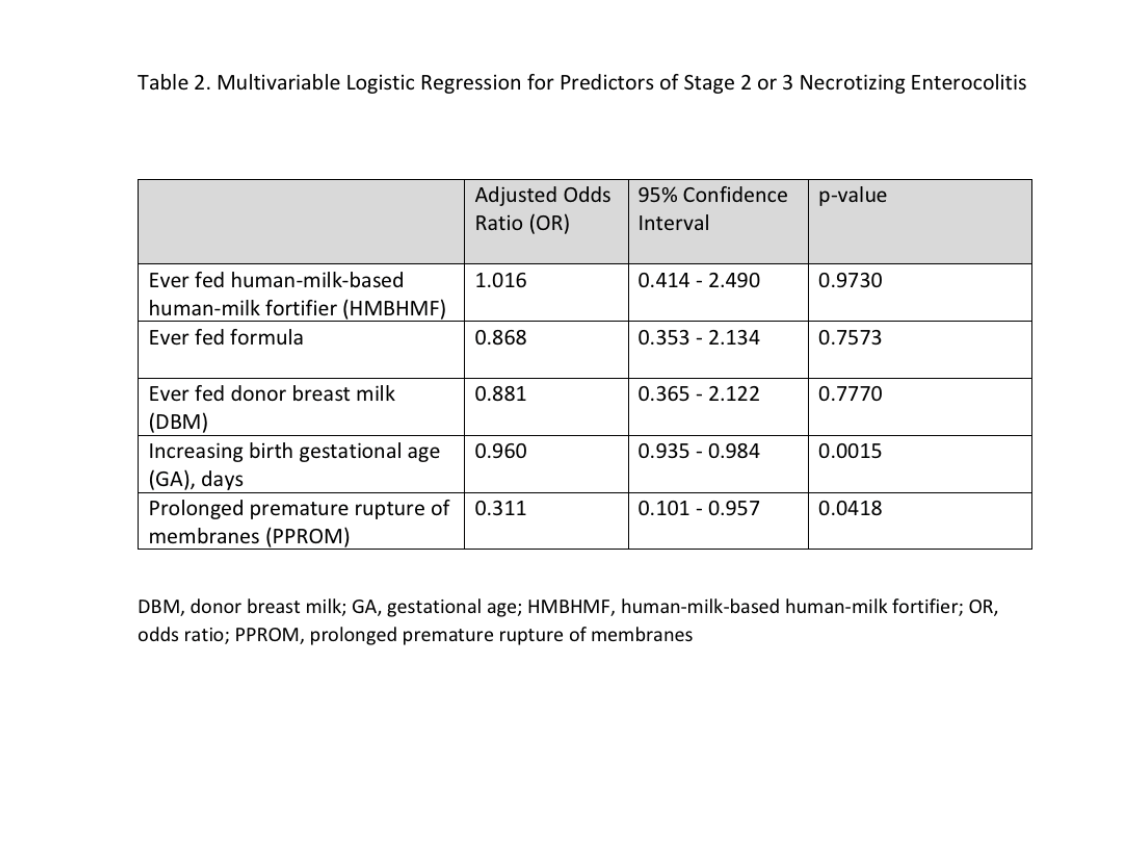 Values adjusted for all variables in the model.
Values adjusted for all variables in the model.