
Nephrology: Clinical
Category: Abstract Submission
Nephrology III: General Nephrology and Dialysis
Daniella Levy Erez, MD, MTR (she/her/hers)
Schneider Children’s Medical Center Israel
Petach Tiqva, HaMerkaz, Israel
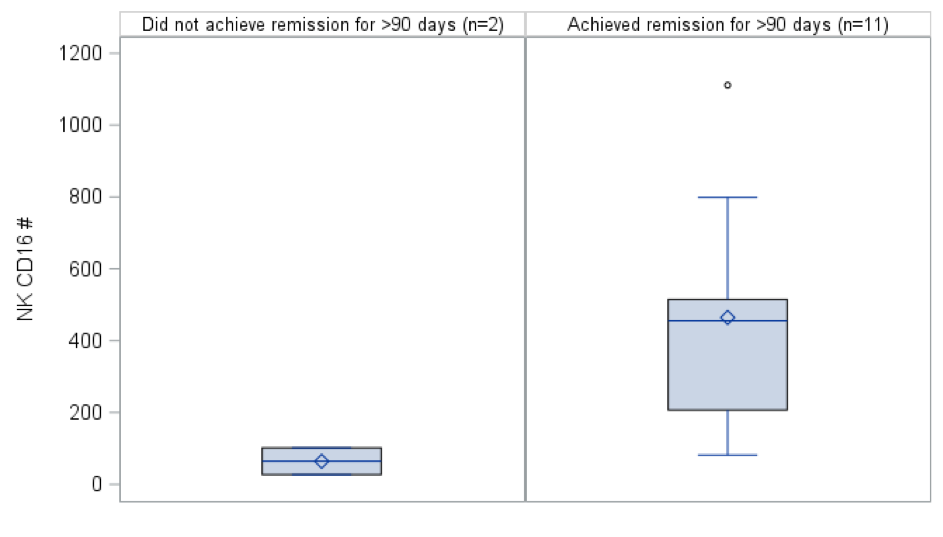 Box plots descriptively compare NK CD16 positive counts pre-rituximab between those who achieved remission for at least 90 days vs. those who did not achieve remission or only achieved remission for ≤90 days for SSNS/SDNS patients.
Box plots descriptively compare NK CD16 positive counts pre-rituximab between those who achieved remission for at least 90 days vs. those who did not achieve remission or only achieved remission for ≤90 days for SSNS/SDNS patients.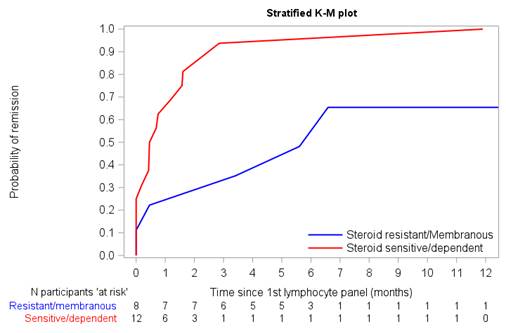 Kaplan Meier curve comparing SRNS/MN and SSNS/SDNS remission probability over time. Higher remission rates with a shorter time to remission were noted among patients with SSNS/SDNS (red) compared to patients with SRNS/MN (blue).
Kaplan Meier curve comparing SRNS/MN and SSNS/SDNS remission probability over time. Higher remission rates with a shorter time to remission were noted among patients with SSNS/SDNS (red) compared to patients with SRNS/MN (blue).