
Breastfeeding/Human Milk
Category: Abstract Submission
Breastfeeding/Human Milk I
 photo")
Erika M. Edwards, PhD, MPH (she/her/hers)
Chief Scientific Officer and Director of Data Science
Vermont Oxford Network
Burlington, Vermont, United States
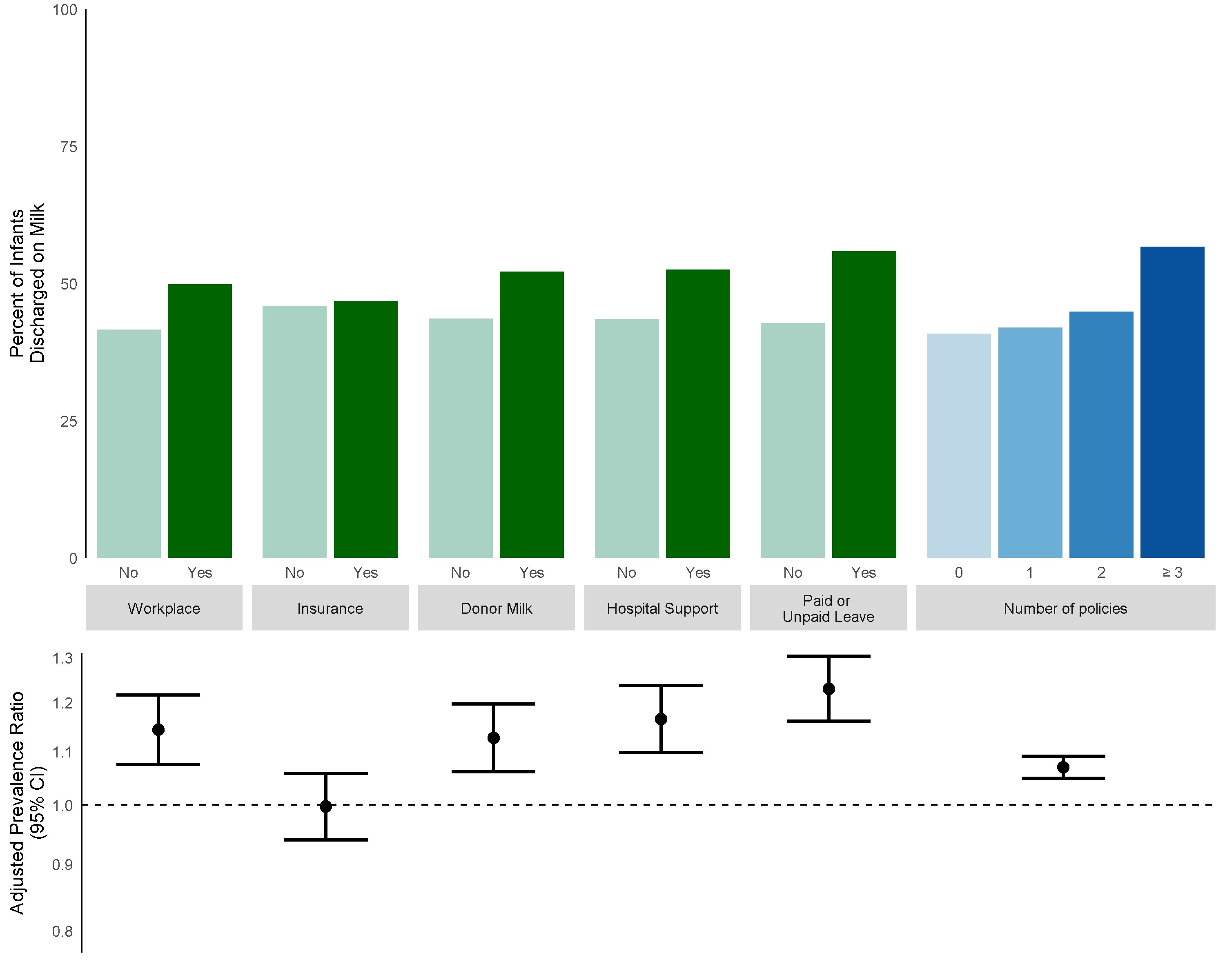 Green bars represent presence or absence of specific types of laws (facilitating breastfeeding the workplace; requiring insurance to cover breastfeeding assistance and training; Medicaid coverage of donor milk; hospital breastfeeding support policies; paid or unpaid medical leave). Blue bars represent total number of policies per state. Prevalence ratios with 95% confidence intervals are adjusted for maternal race/ethnicity.
Green bars represent presence or absence of specific types of laws (facilitating breastfeeding the workplace; requiring insurance to cover breastfeeding assistance and training; Medicaid coverage of donor milk; hospital breastfeeding support policies; paid or unpaid medical leave). Blue bars represent total number of policies per state. Prevalence ratios with 95% confidence intervals are adjusted for maternal race/ethnicity.