151 - Concordance of a Modified Downes’ Score by Physicians and Nurses When Assessing Respiratory Distress Syndrome in the Ethiopian Neonatal Network
Friday, April 22, 2022
6:15 PM – 8:45 PM US MT
Poster Number: 151 Publication Number: 151.112
Danielle Ehret, The University of Vermont Children's Hospital, Burlington, VT, United States; mahlet Abayn, St Paul's Hospital Millennium Medical College, Addis Ababa, Adis Abeba, Ethiopia; Bogale Worku, Ethiopian pediatrics society, addis ababa, Adis Abeba, Ethiopia; Asrat D. Gebremedhin, Tikur Anbessa Specialized Hospital, Addis Ababa, Adis Abeba, Ethiopia; Yohanes M. Hailu, University of Gondar, Gondar, Amara, Ethiopia; Gesit metaferia, St.paul's Hospital Millennium Medical College, Addis Ababa, Adis Abeba, Ethiopia; Kaitlin Kessler, The University of Vermont Children's Hospital, Waterbury Center, VT, United States; Ryan G. Kessler, The University of Vermont Children's Hospital, Waterbury Center, VT, United States; Marie Dunn, St. Michael's Hospital, Toronto, ON, Canada; Jaroslava Belava, Vancouver Coastal Health, Vancouver, BC, Canada; Miroslav Stavel, Royal Columbian Hospital, Vancouver, BC, Canada; Agneta Golan, Soroka Medical Center, Meitar, HaDarom, Israel; Kate Morrow, Vermont Oxford Network, Burlington, VT, United States; Erika M. Edwards, Robert Larner, M.D., College of Medicine at the University of Vermont, Burlington, VT, United States; Jeffrey D. Horbar, Larner College of Medicine University of Vermont, Burlington, VT, United States; Michael S. Dunn, University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada
Associate Professor of Pediatrics The University of Vermont Children's Hospital Burlington, Vermont, United States
Background: Respiratory Distress Syndrome (RDS) is the leading cause of mortality of preterm infants in low- and middle-income countries (LMIC). Lack of diagnostic tools, such as radiography, blood gas analysis, and continuous pulse oximetry along with a scarcity of human resources highlight the need for objective clinical assessments of RDS that can be implemented by multi-disciplinary newborn care providers.
Objective: To assess the correlation of modified Downes’ scores (MDS) assigned by physicians and nurses on admission assessments of preterm infants with RDS in the Ethiopian Neonatal Network (ENN)
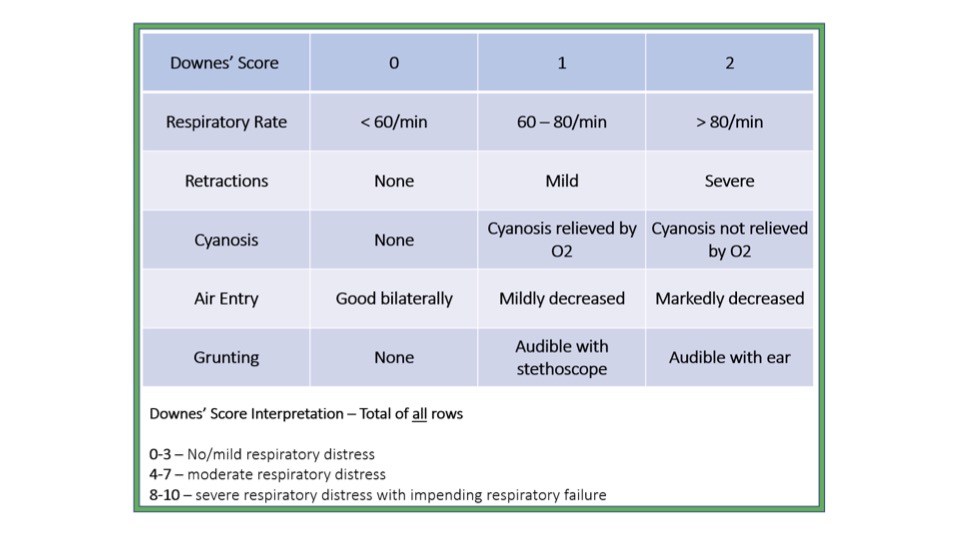
Design/Methods: We included infants with gestational age < 37 weeks with respiratory distress present on admission and treated with oxygen, continuous positive airway pressure (CPAP) or mechanical ventilation within 24 hours and admitted to four tertiary neonatal intensive care units (NICUs) participating in the ENN from June 2019 to June 2020. Nurses and physicians received training on the MDS (Figure), and national guideline for CPAP initiation prompting treatment for scores of 4 or greater combined with an oxygen requirement. The MDS was incorporated into admission assessments, and when feasible, concurrent and independent assessments were completed and recorded by a nurse and physician. We calculated the kappa statistic to determine the nurse and physician correlation for each component of the MDS and the total score, and evaluated the concordance of scores above and below the treatment threshold of 4.
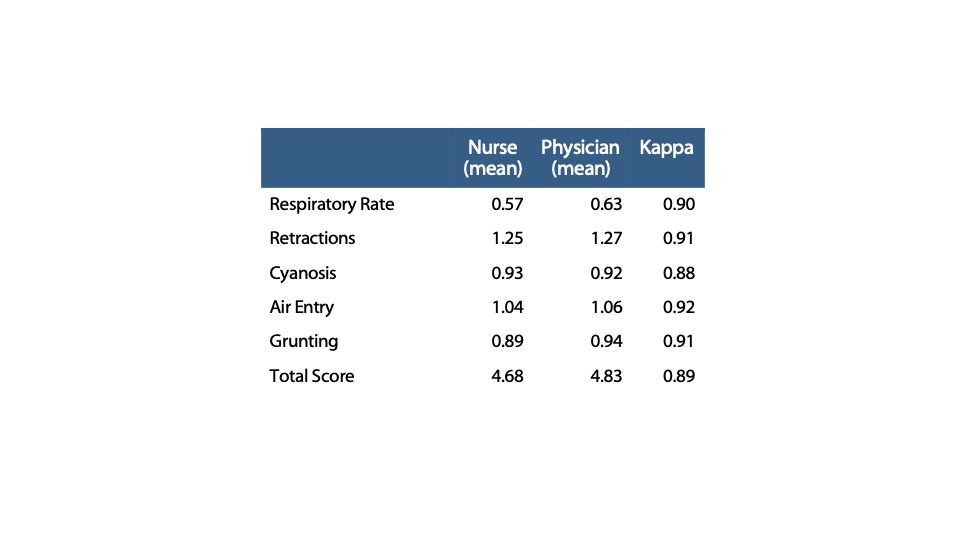
Results: Of the 1016 eligible infants admitted, 1005 (99%) had MDS recorded on admission; 818 infants (81%) had scores reported by nurses; 997 infants (98%) had scores reported by physicians; 817 infants (80%) had scores reported concurrently by both nurses and physicians. The kappa statistic for MDS components ranged from 0.88 to 0.92 and was 0.89 for the total score (Table 1). Of the 817 infants concurrently assessed and scored, 98% had concordance above or below the score-based treatment threshold of 4 (Table 2).Conclusion(s): Incorporation of an objective clinical assessment on admission for preterm infants with RDS was feasible in tertiary NICU settings of the ENN. The kappa statistics of the components of the MDS and total score showed near-perfect agreement between nurse and physician assessments, translating to a very high degree of concordance in score-based treatment recommendations. As LMIC NICUs prioritize improving RDS care and quality of care, these findings reinforce nursing empowerment and task shifting standardized assessments and initiation of CPAP within the context of a multi-disciplinary team. Figure 1. Modified Downes’ score algorithm Table 1. Correlation of modified Downes’ score components and total score as assessed and recorded concurrently and independently by nurses and physicians